
If it feels like many people you know are getting COVID-19 again … you’re not alone.
Fueled by a new subvariant called JN.1, COVID-19 rates are way up for the start of 2024, as part of a sharp rise that began back in November.
So, what do you need to know about the symptoms of JN.1? Is there an updated incubation period to know about for COVID-19 in 2024, and where can you even find a free COVID-19 test now? Keep reading for everything you need to know, or jump straight to:
- What are the symptoms of JN.1?
- What’s the incubation time for COVID-19 now?
- I tested negative. Can I trust my antigen kit?
- Where can I still find free COVID-19 tests?
And remember, the new COVID-19 vaccines from Moderna and Pfizer — and most recently Novavax — are available across California. The new shots are free for everyone, with or without health insurance, and are formulated to target strains like these latest subvariants. Read where to find the new COVID-19 vaccine near you.
What is JN.1, and why is it spreading so much?
Right now, JN.1 is the most prevalent COVID-19 subvariant in the United States, which the Centers for Disease Control and Prevention (CDC) estimates currently makes up almost 62% of cases nationwide. Behind it is the previous top variant, HV.1, which now only makes up 14.8% of cases across the country.
(If you’re losing track of all these subvariants of the omicron variant by this stage of the pandemic, that’s understandable. To recap: The swell of COVID-19 cases in summer 2023 was fueled by EG.5, unofficially nicknamed “Eris” by some online just as XBB.1.16 before it was nicknamed “Arcturus” — even though the World Health Organization has revised its naming conventions to reserve “Greek labels” only for “variants of concern.” After the summer of EG.5, HV.1 rose to national prominence, followed now by JN.1.)
Whereas HV.1 was a part of the XBB sublineage of the omicron variant, JN.1 is closely related to the BA.2.86 strain, the CDC said in an announcement declaring JN.1 “a variant of interest” back in December. And when you’re dealing with descendants like JN.1 and HV.1 before it, it’s important to remember that each new subvariant is more easily transmitted, said Dr. Peter Chin-Hong, an infectious disease expert at UCSF.
“Every time something rises up the charts in the ‘tree of COVID life,’ by essence it had to have a superpower that makes them more powerful than the rest,” Chin-Hong said. “And that superpower is generally transmissibility.”
JN.1’s infectiousness means that the “strategies people could use to escape infection over the summer during our surge are probably not working right now,” Chin-Hong said — added to the fact that winter holidays like Christmas, Hanukkah and New Year prompted travel and brought many people together in crowded gatherings. All of this means that “we all get together, we mix risks from all over the country [and] we don’t have much time to recover before being exposed and exposing others,” Chin-Hong said.
Aside from its infectiousness, the CDC said in its Dec. 8 briefing that there’s “no evidence that JN.1 presents an increased risk to public health relative to other currently circulating variant,” and “no indication of increased severity from JN.1 at this time.”
But, Chin-Hong stressed, JN.1’s increased transmissibility still means that “more people will get infected, which means that our hospitals will be fuller, and that will limit our ability to care for those who have other illnesses.”
What are the symptoms of JN.1?
Chin-Hong confirms that no surprising wild card symptoms have yet been reported for JN.1, or HV.1 before it — they’re the same COVID-19 symptoms you’re used to hearing about from previous variants. Or at least, that’s how it looks right now.
“Like the other omicron flavors,” Chin-Hong said, “many [cases] start with a sore throat,” followed by congestion and a dry cough. From there, “the other symptoms — headache, runny nose, muscle aches, diarrhea or upset stomach, fever, loss of smell— may also join in,” he said.
“The characteristics of the person becoming infected can also shape what symptoms are experienced,” Chin-Hong said, noting that a person age 75 or over or an immunocompromised person who didn’t receive the new COVID-19 vaccine “may experience shortness of breath or difficulty breathing.”
According to the CDC, this is the full list of the possible symptoms of COVID-19:
- Fever or chills
- Cough
- Shortness of breath or difficulty breathing
- Fatigue
- Muscle or body aches
- Headache
- New loss of taste or smell
- Sore throat
- Congestion or runny nose
- Nausea or vomiting
- Diarrhea.
Remember, you might have a combination of these symptoms or just one. They might be mild or feel more severe. But if you’re experiencing any of these, take a COVID-19 test (more on this below).
What are the current COVID-19 cases in the Bay Area right now?
“COVID cases” — that is, positive test results — are not tracked in the way they once were. There’s more on that below, but in the absence of up-to-date widespread data on positive COVID-19 test results, watching for the presence of the coronavirus in human sewage has become increasingly important instead for gauging the levels of COVID-19 spread in a particular area.
Stanford University’s WastewaterSCAN project monitors the presence of COVID-19 — as well as other viruses — in wastewater across the U.S. (For example, you can see the concentration of COVID-19 in wastewater collected from the Oceanside San Francisco watershed.)
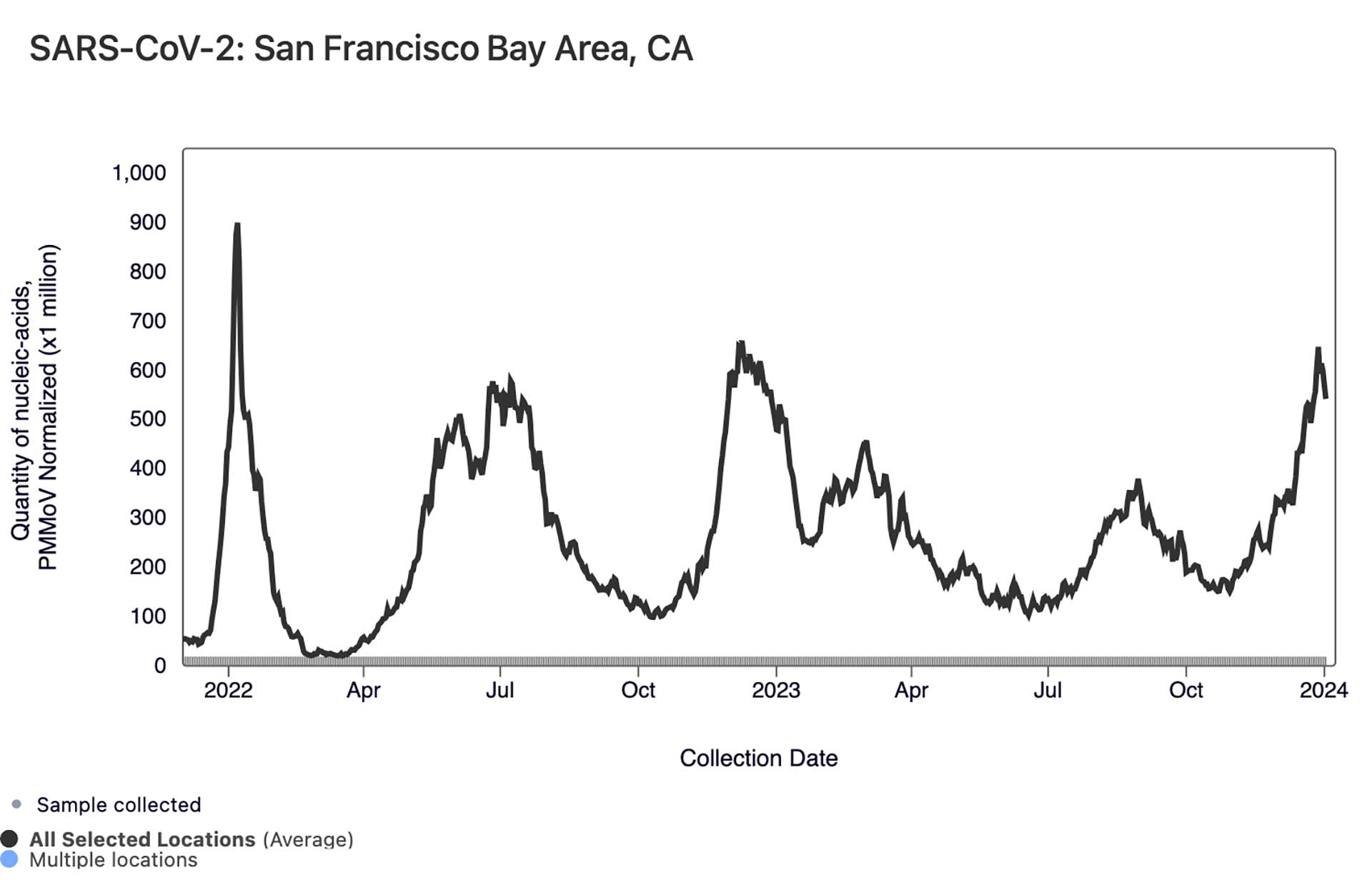
And when it comes to COVID-19 in Bay Area sewage, after numbers came down after that summer swell, WastewaterSCAN’s Ali Boehm told KQED by email on Jan. 8 that those levels of COVID-19 are unfortunately “high and increasing” right now. In the chart below, which shows a trend line aggregated from the Bay Area wastewater sites, you can see how the current rise compares to the highest spike visible, which is the initial omicron surge of winter 2021-22.
As for other winter respiratory viruses, levels of RSV in Bay Area wastewater are “still quite high and have not clearly started decreasing,” Boehm said. One bit of good news: Boehm said that local wastewater shows that the flu is “not circulating now like it did at this time last year.” Read more about the different symptoms of RSV and flu in relation to COVID-19.
Statewide, COVID-19 metrics are also back on the upswing after a lull. The state’s 7-day COVID-19 positivity test rate tracks the average percentage of people in California each week who get a positive diagnostic test result from a lab after taking a PCR test. The statewide positivity rate reached its highest point for the entire year back on Sept. 2, at 17.4%.
But after falling to a low of 6.1% on Nov. 3, the weekly average positivity rate has climbed again to 12.3% as of the most recently available data, collected on Jan. 1. (It’s worth noting that many people who suspect they have COVID-19 in 2023 test themselves at home with an antigen test kit, not a PCR test — so this tracking from the California Department of Public Health doesn’t represent the full picture of COVID-19 positivity around the state.)
After a lull following the 2023 summer swell, the number of people hospitalized with COVID-19 in California began climbing again in November and peaked on Dec. 22 with a 7-day average of 2,339 people hospitalized statewide. The most recent available data, from Dec. 31, shows a drop to a 7-day average of 1,990 patients.

