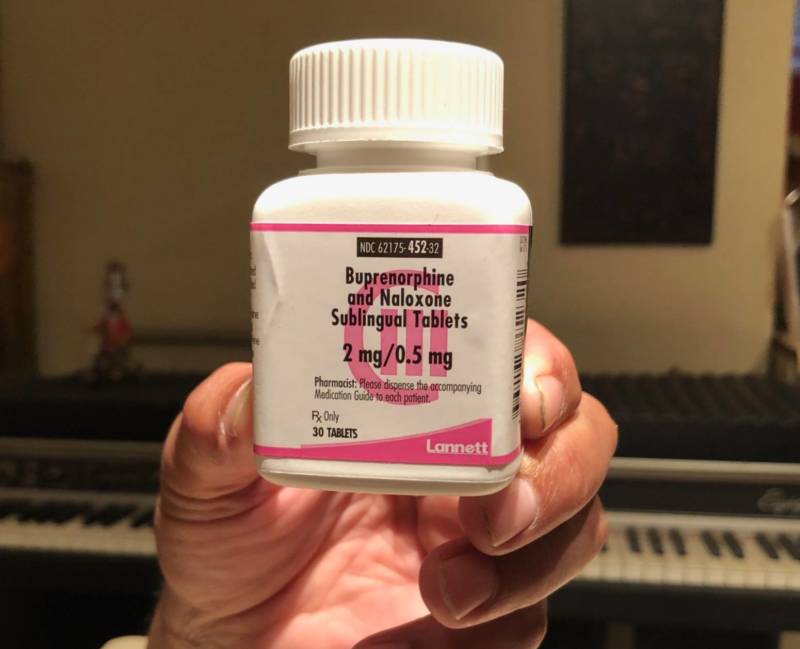
Each morning when Tomás wakes up, he opens his nightstand drawer and takes his medications: a drug for high blood pressure, pain relievers for his sciatica and a light pink pill.
The 68-year-old places the pill under his tongue and waits for it to dissolve.
"It has a typical medicinal taste to it," Tomás said. "It's just slightly bitter."
The medication is buprenorphine. It's a prescription drug that curbs the cravings that come from opioid addiction. When dosed correctly, it won't produce a high.
Tomás is one of a growing number of Californians with prescriptions for buprenorphine, one of the FDA-approved drugs that is part of medication-assisted treatment (MAT) for opioid addiction. MAT combines those medications with counseling and is considered the most effective way to treat opioid addiction.
While the opioid crisis has not hit California as hard as some of the Eastern states, roughly 2,000 Californians die each year of an opioid overdose.
In a bid to combat this, California's Department of Health Care Services (DHCS) has invested $265 million since 2017 to increase access to medication-assisted treatment throughout the state.
Tomás' story offers a window into what America's opioid crisis may look like in the future: people on medication to treat their addiction for years, or even for the rest of their lives.
'I Can Control This'
Tomás was once addicted to heroin, and preferred only his first name be used in this article. He owns a landscaping business and is concerned that current or future clients may peg him as untrustworthy if they learn about his past.
He started using heroin at 18, when he was in the Army during the Vietnam War. He was stationed in Germany.
"I didn't think much of it at the time, thinking I can control this, this won't be a problem," Tomás said. "That when I get out of the service I'll just put this behind me."
But things didn't pan out that way, and Tomás continued seeking out and using heroin. He said he hit bottom in the 1980s when he was back living in the U.S.
"I was a dealer-addict," Tomás said. He lived in San Francisco's Mission District, "in one of those fleabag hotels. I had a girlfriend who was a working girl. We slung dope, and did a lot of dope."
He said that life was dangerous and lonely, and eventually he wanted something different.
"I just woke up to my surroundings one morning and realized, this isn’t the way to live," he said.
Tomás got clean with the help of methadone, another medication for opioid addiction. Eventually, though, he chose to stop taking it. He liked the idea of being free of any medications, and he said the methadone made him sleepy and turned his thinking a bit cloudy.