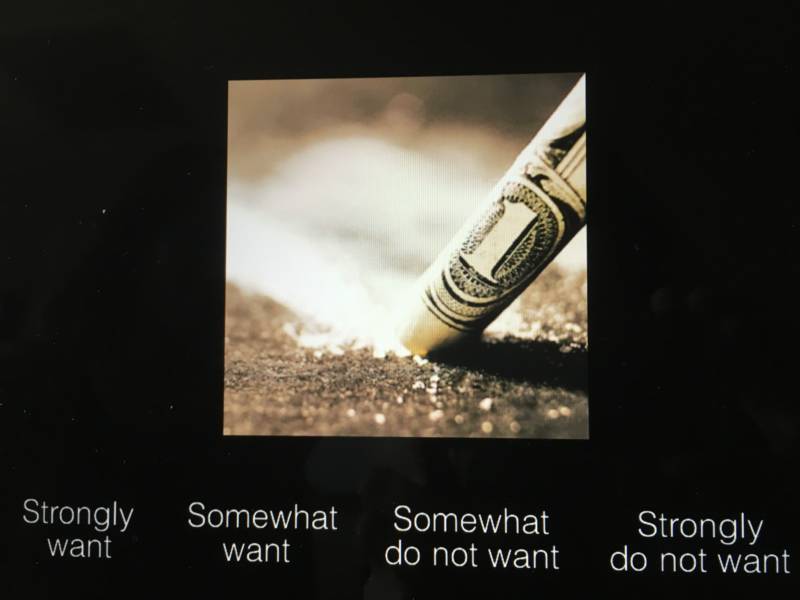
Participants in an ongoing study on drug relapse at Stanford rate their desire for the contents of images like these, while researchers record what's happening in their brains. (April Dembosky/KQED)
Dee Dee is lying on her back, the cacophony of the MRI machine’s ringing and buzzing all around her head.
She stares straight up at a mirror that’s tilted so she can see a computer screen at her feet. It projects a series of images: a glass of beer, a piece of pizza, a line of methamphetamine. In her hands, she holds the controls to indicate, on a scale of 1 to 4, how much she wants what’s in the picture.
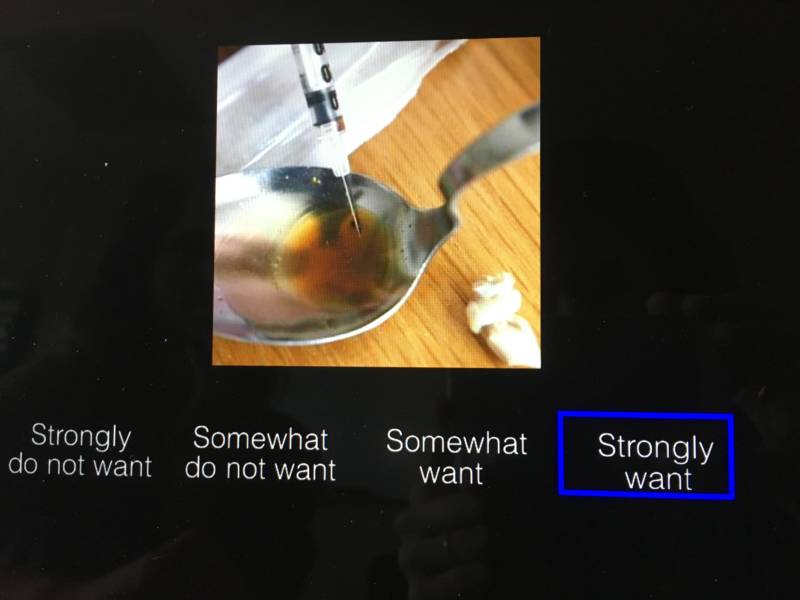
The more detailed the photos became, the more she wanted what was in them, she said later. A bag of white powder? No big deal. But a needle, with speed in it, ready to inject? That was different.
“The interest went from, ‘No? No.’ To just all of a sudden, ‘Yeah, yeah, yeah,’ ” she says. “Just thinking about it right now, I can kind of taste it in the back of my throat.”
A team of researchers at Stanford University are scanning the brains of stimulant users like Dee Dee to better understand one of the most intractable and frustrating questions in addiction treatment: Who is most likely to relapse and why? Current studies show that 60 percent of people in rehab for meth addiction relapse within a year of discharge, a stat that has health officials on edge as meth use in San Francisco is again surging.
Sponsored
Neuropsychologist Kelly MacNiven and her team believe they may have identified a signal in the brain that can predict who will relapse.
“We can potentially use this to see who is at greater risk for relapse,” MacNiven says. “We can also potentially try to develop better interventions that target this brain activity, and we can see if by reducing this brain activity, if that can reduce relapse risk.”
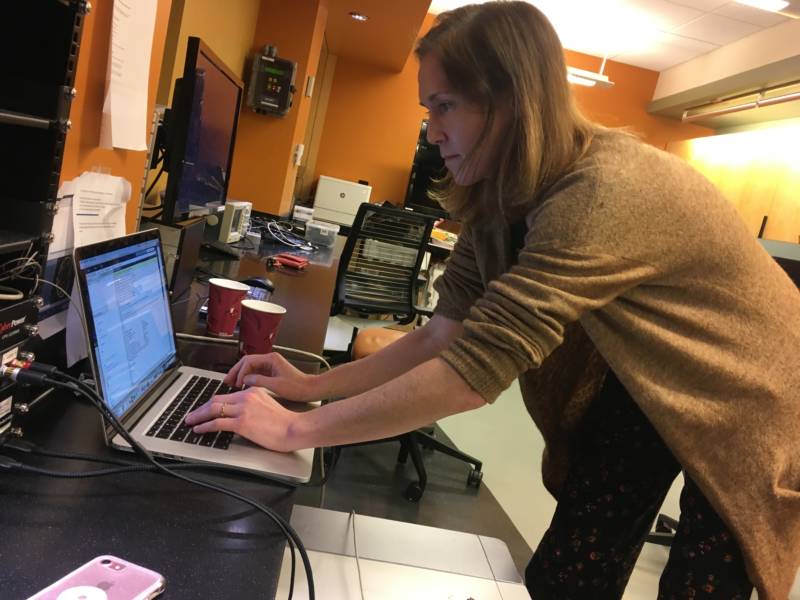
Neuropsychologist Kelly MacNiven sets up the MRI scanner at Stanford. (April Dembosky/KQED)
While test subjects like Dee Dee look at pictures in the MRI scanner, MacNiven sits on the other side of the wall, looking at the brain scans on her computer screen. When all the scans are complete, the teams goes over them, specifically studying the nucleus accumbens, located in the middle of the brain.
In their first round of the scanning study, MacNiven’s team found that the people whose brains really light up in this spot when they’re looking at the pictures of meth and cocaine are the ones most likely to relapse. Six months after the scan, they were twice as likely to have used again.
“This suggests, if this replicates, that we have a brain signal that basically is related to relapse,” says MacNiven, a postdoc fellow in the psychology department at Stanford and lead author of the study.
Confronting Relapse
Dee Dee was 14 when she tried methamphetamine for the first time. Her parents had recently gotten divorced.
“My family, in the blink of an eye, was torn apart and I didn’t understand it,” says Dee Dee, who asked that we not reveal her last name. “I remember just being really broken."
She had to move, and the kids she became friends with were experimenting with all kinds of drugs. But she liked meth the best.
“When I smoked pot, it made me hungry and it just made me really tired. Meth was the total opposite, I had energy,” she says. “Me and my friends, we went from like not wanting to do anything to just like wanting to clean, and like, kind of like you feel like you're being productive.”
She used on and off for years, then went into treatment when she was 26. She met a guy there. They got sober together and had a baby. Then he relapsed. And then Dee Dee relapsed. She was using meth every day.
“My line of work was high sales, so I had to always have my A-game on,” she says. “Even when I was really tired from being a young mom, it gave me energy to do everything.”
Within four months, Dee Dee lost her job, her apartment, her car. Now she’s in treatment again, trying to understand what it was about last time that didn’t stick.
“I just don’t want to be in and out of treatment centers. I want to get it right,” she says.
Dopamine Versus Self-report
Relapse most often results from a trigger in the user’s environment: driving past the bar they used to go to in order to get high, the smell of a certain cigarette or running into someone they used to use with.
This is what researchers are trying to emulate in the MRI lab, by showing pictures of drug paraphernalia to elicit the same response in the brain.
MacNiven and her team believe dopamine is at work here: Before a person has smoked or snorted any drug, the brain releases a bit of dopamine in anticipation of getting high.
“Addictive drugs are in some way hijacking the dopamine system,” MacNiven says.
They do this in two ways. First, there’s the dopamine response to the meth itself that makes a person feel really, really good. Second, there’s a kind of learned behavior, a trained dopamine release at the sight of the meth, or the old bar or friend — this is the brain teaching itself what behaviors lead to the ingestion of the drug that feels so good.
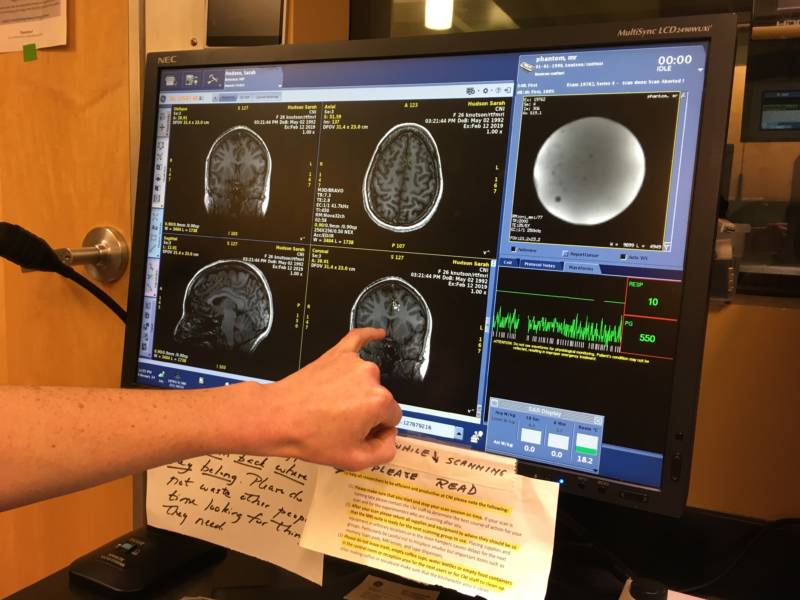
MacNiven points to the nucleus accumbens. People who showed the most activity in this part of the brain while looking at images of drugs were the most likely to relapse. (April Dembosky/KQED)
In animal studies, this anticipatory dopamine release goes straight to the nucleus accumbens in the middle of the brain. The Stanford study is the first to replicate this in humans.
They believe this brain marker is a much more robust, dependable predictor of who will relapse, as opposed to users reporting cravings or environmental triggers. The study showed that users themselves cannot predict their own likelihood of relapse.
So even though Dee Dee could taste drugs in the back of her throat when thinking about pictures of dope, in the end, that may have no bearing on her risk of relapse. In MacNiven’s first round of tests, what former drug users said they wanted had no relation to what their brains said they wanted, MacNiven says. Self-reports did not predict who ended up relapsing and who didn’t. Only the brain activity did.
“We actually think this is interesting and might be a factor related to addiction, meaning that you might not have the ability to really know what you want,” MacNiven says.
To be sure of this conclusion, researchers have to test more people. They did the first round of scans on veterans — almost all men. Historically, this is true of a lot of addiction research. MacNiven is now actively recruiting and testing women to make sure her results hold up.
“This confirmation is vital, as women with stimulant use disorders may have more intense craving after drug cessation,” wrote Jay Nierenberg, a psychiatry professor at NYU School of Medicine, in a paper reviewing the Stanford results among vets. “And poorer clinical outcomes among women with stimulant use disorders have been reported in multiple studies.”
What former users said they wanted had no bearing on whether they went on to relapse. (April Dembosky/KQED)
Implications for Treatment
If the findings do hold up in a larger, more diverse population, the implications could be powerful. Treatment providers could tailor care more specifically and target more precisely who should get what kind of treatment and for how long.
“Identifying those at greatest risk and providing treatment that specifically targets modifiable components of that risk would undoubtedly change the landscape of substance abuse treatment, likely attracting more people who need it and perhaps reducing burnout among those who provide it,” Nierenberg writes.
But it also means the only way to know who’s at highest risk for relapse requires giving everyone an MRI.
“I would say, is that so bad?” MacNiven asks. “Doing a $400 MRI scan, if that actually keeps people from relapsing, then I would say that it’s worth it.”
But of course getting access to this kind of diagnostic care is much more complicated than that. Not everyone who needs help with relapse lives near Stanford, or any MRI lab, and the details of this experiment are complex and difficult to emulate in other clinical settings. Plus, the scans take six hours for each test subject — not everyone can tolerate being enclosed in a tight, noisy machine for that long.
"These results help to advance the field, although use in clinical practice is unlikely, at least for the time being," says Dr. Phillip Coffin, director of substance use research at the San Francisco Department of Public Health.
Then there is the question of effective treatments. There are no Food and Drug Administration-approved medications for stimulant addiction the way there are for opioids.
MacNiven and her team are brainstorming other options from their research — things like magnetic stimulation of the scalp to interfere with the brain’s addiction activity. Or neurofeedback, where users train their own brains not to light up at the sight of drugs.
“The idea that there could be anything that is an option for people, that is not the conventional standard stuff, is really exciting to people,” MacNiven says, “even if it’s something like brain zapping.”
That would be a relief to folks like Dee Dee. She’s been in treatment for four months so far at the Epiphany Center, a residential program for women in San Francisco. She admits her initial interest in participating in the study was for the free lunch and the Amazon gift card. But that changed the more she understood the research goals.
Sponsored
“Anything that I can use to help people understand why we do the things we do, or maybe help someone to say no to drugs?” she says, “I'm all for it.”
lower waypoint
Stay in touch. Sign up for our daily newsletter.
To learn more about how we use your information, please read our privacy policy.
window.__IS_SSR__=true
window.__INITIAL_STATE__={"attachmentsReducer":{"audio_0":{"type":"attachments","id":"audio_0","imgSizes":{"kqedFullSize":{"file":"https://ww2.kqed.org/news/wp-content/themes/KQED-unified/img/audio_bgs/background0.jpg"}}},"audio_1":{"type":"attachments","id":"audio_1","imgSizes":{"kqedFullSize":{"file":"https://ww2.kqed.org/news/wp-content/themes/KQED-unified/img/audio_bgs/background1.jpg"}}},"audio_2":{"type":"attachments","id":"audio_2","imgSizes":{"kqedFullSize":{"file":"https://ww2.kqed.org/news/wp-content/themes/KQED-unified/img/audio_bgs/background2.jpg"}}},"audio_3":{"type":"attachments","id":"audio_3","imgSizes":{"kqedFullSize":{"file":"https://ww2.kqed.org/news/wp-content/themes/KQED-unified/img/audio_bgs/background3.jpg"}}},"audio_4":{"type":"attachments","id":"audio_4","imgSizes":{"kqedFullSize":{"file":"https://ww2.kqed.org/news/wp-content/themes/KQED-unified/img/audio_bgs/background4.jpg"}}},"placeholder":{"type":"attachments","id":"placeholder","imgSizes":{"thumbnail":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-160x96.jpg","width":160,"height":96,"mimeType":"image/jpeg"},"medium":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-800x478.jpg","width":800,"height":478,"mimeType":"image/jpeg"},"large":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-1020x610.jpg","width":1020,"height":610,"mimeType":"image/jpeg"},"fd-lrg":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-1920x1148.jpg","width":1920,"height":1148,"mimeType":"image/jpeg"},"fd-med":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-1180x705.jpg","width":1180,"height":705,"mimeType":"image/jpeg"},"fd-sm":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-960x574.jpg","width":960,"height":574,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"xxsmall":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-240x143.jpg","width":240,"height":143,"mimeType":"image/jpeg"},"xsmall":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-375x224.jpg","width":375,"height":224,"mimeType":"image/jpeg"},"small":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-520x311.jpg","width":520,"height":311,"mimeType":"image/jpeg"},"xlarge":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-1180x705.jpg","width":1180,"height":705,"mimeType":"image/jpeg"},"full-width":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-1920x1148.jpg","width":1920,"height":1148,"mimeType":"image/jpeg"},"guest-author-32":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-32x32.jpg","width":32,"height":32,"mimeType":"image/jpeg"},"guest-author-50":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-50x50.jpg","width":50,"height":50,"mimeType":"image/jpeg"},"guest-author-64":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-64x64.jpg","width":64,"height":64,"mimeType":"image/jpeg"},"guest-author-96":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-96x96.jpg","width":96,"height":96,"mimeType":"image/jpeg"},"guest-author-128":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-128x128.jpg","width":128,"height":128,"mimeType":"image/jpeg"},"detail":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-150x150.jpg","width":150,"height":150,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://ww2.kqed.org/wp-content/uploads/sites/10/2018/01/GettyImages-896326950-e1514998105161.jpg","width":1920,"height":1148}}},"news_11976827":{"type":"attachments","id":"news_11976827","meta":{"index":"attachments_1591205162","site":"news","id":"11976827","found":true},"title":"240215-PRESCHOOLSUSPENSION-24-BL-KQED","publishDate":1708641117,"status":"inherit","parent":0,"modified":1713225146,"caption":"Danielle Jorgenson, known to students as Teacher Dani, works with students in a garden during a preschool class at Los Medanos College Child Study Center in Pittsburg, California, on Feb. 15, 2024.","credit":"Beth LaBerge/KQED","altTag":null,"description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-1536x1024.jpg","width":1536,"height":1024,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED-1920x1280.jpg","width":1920,"height":1280,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-24-BL-KQED.jpg","width":2000,"height":1333}},"fetchFailed":false,"isLoading":false},"news_11965073":{"type":"attachments","id":"news_11965073","meta":{"index":"attachments_1591205162","site":"news","id":"11965073","found":true},"title":"231017-LakeMercedRVs-021-BL-KQED","publishDate":1697758895,"status":"inherit","parent":0,"modified":1713305461,"caption":"RVs line Winston Drive in San Francisco on Oct. 17, 2023, near San Francisco State University.","credit":"Beth LaBerge/KQED","altTag":"A row of RVs parked along a two-lane street.","description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-1536x1024.jpg","width":1536,"height":1024,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED-1920x1280.jpg","width":1920,"height":1280,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-021-BL-KQED.jpg","width":2000,"height":1333}},"fetchFailed":false,"isLoading":false},"news_11983111":{"type":"attachments","id":"news_11983111","meta":{"index":"attachments_1591205162","site":"news","id":"11983111","found":true},"title":"240415-OAKLAND ROOTS-KQED","publishDate":1713289800,"status":"inherit","parent":0,"modified":1713295573,"caption":"Despite playing in different leagues, San Francisco's El Farolito soccer team (in yellow and blue kits) will face off against the Oakland Roots on Tuesday, April 16, 2024, thanks to U.S. Open Cup rules. The Roots beat El Farolito at last year's Open Cup second-round match on April 4, 2023, pictured above, and El Farolito head coach Santiago López says his players are looking forward to a rematch.","credit":"Courtesy of Oakland Roots SC","altTag":"Three men wearing soccer equipment and kits play on a field with a goalie in the background.","description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-1536x1024.jpg","width":1536,"height":1024,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED-1920x1280.jpg","width":1920,"height":1280,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-OAKLAND-ROOTS-KQED.jpg","width":2000,"height":1333}},"fetchFailed":false,"isLoading":false},"news_11983218":{"type":"attachments","id":"news_11983218","meta":{"index":"attachments_1591205162","site":"news","id":"11983218","found":true},"title":"CMHospitals01","publishDate":1713372118,"status":"inherit","parent":11983217,"modified":1713380198,"caption":"A newborn baby at Martin Luther King Community Hospital in Los Angeles on March 22, 2024.","credit":"Jules Hotz/CalMatters","altTag":null,"description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-1536x1024.jpg","width":1536,"height":1024,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01-1920x1280.jpg","width":1920,"height":1280,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMHospitals01.jpg","width":2000,"height":1333}},"fetchFailed":false,"isLoading":false},"forum_2010101905423":{"type":"attachments","id":"forum_2010101905423","meta":{"index":"attachments_1591205162","site":"forum","id":"2010101905423","found":true},"title":"99 Cents Only Stores storefront and parking lot in Houston, TX.","publishDate":1713310715,"status":"inherit","parent":2010101905416,"modified":1713311015,"caption":"99 Cents Only Stores storefront and parking lot.","credit":"Brent Hondow via Getty Images","altTag":"99 Cents Only storefront","description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"medium_large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601-768x512.jpg","width":768,"height":512,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/iStock-1363890601.jpg","width":1254,"height":836}},"fetchFailed":false,"isLoading":false},"news_11983184":{"type":"attachments","id":"news_11983184","meta":{"index":"attachments_1591205162","site":"news","id":"11983184","found":true},"title":"CMEncampmentBan01","publishDate":1713311401,"status":"inherit","parent":11983180,"modified":1713311436,"caption":"An encampment is seen on the sidewalk near a freeway entrance in downtown San Diego on March 22, 2024. Unhoused individuals moved their belongings across the street and later came back after cleaning finished.","credit":"Kristian Carreon/CalMatters","altTag":null,"description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-1536x1024.jpg","width":1536,"height":1024,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01-1920x1280.jpg","width":1920,"height":1280,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/CMEncampmentBan01.jpg","width":2000,"height":1333}},"fetchFailed":false,"isLoading":false},"news_11983025":{"type":"attachments","id":"news_11983025","meta":{"index":"attachments_1591205162","site":"news","id":"11983025","found":true},"title":"GettyImages-623874284_qut","publishDate":1713210545,"status":"inherit","parent":11983000,"modified":1713214063,"caption":"A worker stands on the roof of a home under construction at a new housing development on Nov. 17, 2016, in San Rafael. ","credit":"Justin Sullivan/Getty Images","altTag":"A person wearing construction equipment holds a wooden support beam while a roof is built.","description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-800x553.jpg","width":800,"height":553,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-1020x705.jpg","width":1020,"height":705,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-160x111.jpg","width":160,"height":111,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-1536x1062.jpg","width":1536,"height":1062,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut.jpg","width":1920,"height":1327}},"fetchFailed":false,"isLoading":false},"forum_2010101905412":{"type":"attachments","id":"forum_2010101905412","meta":{"index":"attachments_1591205162","site":"forum","id":"2010101905412","found":true},"title":"GettyImages-2147864229 (1)","publishDate":1713307416,"status":"inherit","parent":2010101905411,"modified":1713308050,"caption":"Supporters cheer during a public rally addressed by Prime Minister Narendra Modi, ahead of the upcoming Lok Sabha election on April 16, 2024 in Gaya, India.","credit":"Hindustan Times via Getty Images","altTag":null,"description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-800x450.jpg","width":800,"height":450,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-1020x574.jpg","width":1020,"height":574,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-160x90.jpg","width":160,"height":90,"mimeType":"image/jpeg"},"medium_large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-768x432.jpg","width":768,"height":432,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-1536x864.jpg","width":1536,"height":864,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/43/2024/04/GettyImages-2147864229-1.jpg","width":1920,"height":1080}},"fetchFailed":false,"isLoading":false},"news_11983214":{"type":"attachments","id":"news_11983214","meta":{"index":"attachments_1591205162","site":"news","id":"11983214","found":true},"title":"riverside-county-661fd0e65ff86","publishDate":1713361159,"status":"inherit","parent":11983211,"modified":1713361256,"caption":"Lisa Matus speaks at a news conference on in-custody jail deaths in Riverside County.","credit":"Madison Aument/KVCR","altTag":"Riverside County Jail Deaths","description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86-800x572.jpg","width":800,"height":572,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86-1020x729.jpg","width":1020,"height":729,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86-160x114.jpg","width":160,"height":114,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86-1536x1098.jpg","width":1536,"height":1098,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/riverside-county-661fd0e65ff86.jpg","width":1760,"height":1258}},"fetchFailed":false,"isLoading":false},"news_11983294":{"type":"attachments","id":"news_11983294","meta":{"index":"attachments_1591205162","site":"news","id":"11983294","found":true},"title":"240408-FCIDublin-018-BL_qut","publishDate":1713395313,"status":"inherit","parent":11983285,"modified":1713398577,"caption":"The Federal Correctional Institution, Dublin, a prison for women on April 8, 2024.","credit":"Beth LaBerge/KQED","altTag":"A photo of a large prison behind a fence.","description":null,"imgSizes":{"medium":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut-800x533.jpg","width":800,"height":533,"mimeType":"image/jpeg"},"large":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut-1020x680.jpg","width":1020,"height":680,"mimeType":"image/jpeg"},"thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut-160x107.jpg","width":160,"height":107,"mimeType":"image/jpeg"},"1536x1536":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut-1536x1024.jpg","width":1536,"height":1024,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240408-FCIDublin-018-BL_qut.jpg","width":1920,"height":1280}},"fetchFailed":false,"isLoading":false},"news_11728942":{"type":"attachments","id":"news_11728942","meta":{"index":"attachments_1591205162","site":"news","id":"11728942","found":true},"title":"Stanford study coke","publishDate":1551146221,"status":"inherit","parent":11728856,"modified":1551196455,"caption":"Participants in an ongoing study on drug relapse at Stanford rate their desire for the contents of images like these, while researchers record what's happening in their brains.","credit":"April Dembosky/KQED","description":null,"imgSizes":{"thumbnail":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-160x120.jpg","width":160,"height":120,"mimeType":"image/jpeg"},"medium":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-800x600.jpg","width":800,"height":600,"mimeType":"image/jpeg"},"large":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-1020x765.jpg","width":1020,"height":765,"mimeType":"image/jpeg"},"complete_open_graph":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-1200x900.jpg","width":1200,"height":900,"mimeType":"image/jpeg"},"post-thumbnail":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-672x372.jpg","width":672,"height":372,"mimeType":"image/jpeg"},"twentyfourteen-full-width":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-1038x576.jpg","width":1038,"height":576,"mimeType":"image/jpeg"},"full-width":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-1920x1440.jpg","width":1920,"height":1440,"mimeType":"image/jpeg"},"guest-author-32":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-32x32.jpg","width":32,"height":32,"mimeType":"image/jpeg"},"guest-author-50":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-50x50.jpg","width":50,"height":50,"mimeType":"image/jpeg"},"guest-author-64":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-64x64.jpg","width":64,"height":64,"mimeType":"image/jpeg"},"guest-author-96":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-96x96.jpg","width":96,"height":96,"mimeType":"image/jpeg"},"guest-author-128":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-128x128.jpg","width":128,"height":128,"mimeType":"image/jpeg"},"detail":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-150x150.jpg","width":150,"height":150,"mimeType":"image/jpeg"},"kqedFullSize":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-e1551146243498.jpg","width":1920,"height":1440}},"fetchFailed":false,"isLoading":false}},"audioPlayerReducer":{"postId":"stream_live"},"authorsReducer":{"byline_news_11983217":{"type":"authors","id":"byline_news_11983217","meta":{"override":true},"slug":"byline_news_11983217","name":"Kristen Hwang, CalMatters","isLoading":false},"byline_news_11983180":{"type":"authors","id":"byline_news_11983180","meta":{"override":true},"slug":"byline_news_11983180","name":"Marisa Kendall, CalMatters","isLoading":false},"kqed":{"type":"authors","id":"236","meta":{"index":"authors_1591205172","id":"236","found":true},"name":"KQED News Staff","firstName":"KQED News Staff","lastName":null,"slug":"kqed","email":"faq@kqed.org","display_author_email":false,"staff_mastheads":[],"title":null,"bio":null,"avatar":"https://secure.gravatar.com/avatar/ef0e801a68c4c54afa9180db14084167?s=600&d=blank&r=g","twitter":null,"facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"arts","roles":["contributor"]},{"site":"news","roles":["editor"]},{"site":"futureofyou","roles":["author"]}],"headData":{"title":"KQED News Staff | KQED","description":null,"ogImgSrc":"https://secure.gravatar.com/avatar/ef0e801a68c4c54afa9180db14084167?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/ef0e801a68c4c54afa9180db14084167?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/kqed"},"minakim":{"type":"authors","id":"243","meta":{"index":"authors_1591205172","id":"243","found":true},"name":"Mina Kim","firstName":"Mina","lastName":"Kim","slug":"minakim","email":"mkim@kqed.org","display_author_email":false,"staff_mastheads":["news"],"title":"Host, Forum","bio":"Mina Kim is host of the 10 a.m. statewide hour of Forum; a live daily talk show for curious Californians on issues that matter to the state and nation, with a particular emphasis on race and equity.\r\n\r\nBefore joining the Forum team, Mina was KQED’s evening news anchor, and health reporter for The California Report. Her award-winning work has included natural disasters in Napa and gun violence in Oakland. Mina grew up in St. John’s, Newfoundland.","avatar":"https://secure.gravatar.com/avatar/145ce657a2d08cb86d93686beb958982?s=600&d=blank&r=g","twitter":"mkimreporter","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"news","roles":["contributor"]},{"site":"stateofhealth","roles":["author"]},{"site":"forum","roles":["editor"]}],"headData":{"title":"Mina Kim | KQED","description":"Host, Forum","ogImgSrc":"https://secure.gravatar.com/avatar/145ce657a2d08cb86d93686beb958982?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/145ce657a2d08cb86d93686beb958982?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/minakim"},"ahall":{"type":"authors","id":"11490","meta":{"index":"authors_1591205172","id":"11490","found":true},"name":"Alex Hall","firstName":"Alex","lastName":"Hall","slug":"ahall","email":"ahall@kqed.org","display_author_email":false,"staff_mastheads":["news"],"title":"KQED Enterprise & Accountability Reporter","bio":"Alex Hall is KQED's Enterprise and Accountability Reporter. She previously covered the Central Valley for five years from KQED's bureau in Fresno. Before joining KQED, Alex was an investigative reporting fellow at Wisconsin Public Radio and the Wisconsin Center for Investigative Journalism. She has also worked as a bilingual producer for NPR's investigative unit and freelance video producer for Reuters TV on the Latin America desk. She got her start in journalism in South America, where she worked as a radio producer and Spanish-English translator for CNN Chile. Her documentary and investigation into the series of deadly COVID-19 outbreaks at Foster Farms won a national Edward R. Murrow award and was named an Investigative Reporters & Editors award finalist. Alex's reporting for Reveal on the Wisconsin dairy industry's reliance on undocumented immigrant labor was made into a film, Los Lecheros, which won a regional Edward R. Murrow award for best news documentary.","avatar":"https://secure.gravatar.com/avatar/defcbeb88b0bf591ff9af41f22644051?s=600&d=blank&r=g","twitter":"@chalexhall","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"news","roles":["editor"]}],"headData":{"title":"Alex Hall | KQED","description":"KQED Enterprise & Accountability Reporter","ogImgSrc":"https://secure.gravatar.com/avatar/defcbeb88b0bf591ff9af41f22644051?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/defcbeb88b0bf591ff9af41f22644051?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/ahall"},"abandlamudi":{"type":"authors","id":"11672","meta":{"index":"authors_1591205172","id":"11672","found":true},"name":"Adhiti Bandlamudi","firstName":"Adhiti","lastName":"Bandlamudi","slug":"abandlamudi","email":"abandlamudi@kqed.org","display_author_email":false,"staff_mastheads":["news"],"title":"KQED Housing Reporter","bio":"Adhiti Bandlamudi reports for KQED's Housing desk. She focuses on how housing gets built across the Bay Area. Before joining KQED in 2020, she reported for WUNC in Durham, North Carolina, WABE in Atlanta, Georgia and Capital Public Radio in Sacramento. In 2017, she was awarded a Kroc Fellowship at NPR where she reported on everything from sprinkles to the Golden State Killer's arrest. When she's not reporting, she's baking new recipes in her kitchen or watching movies with friends and family. She's originally from Georgia and has strong opinions about Great British Bake Off.","avatar":"https://secure.gravatar.com/avatar/868129c8b257bb99a3500e2c86a65400?s=600&d=blank&r=g","twitter":"oddity_adhiti","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"arts","roles":["author"]},{"site":"news","roles":["editor"]}],"headData":{"title":"Adhiti Bandlamudi | KQED","description":"KQED Housing Reporter","ogImgSrc":"https://secure.gravatar.com/avatar/868129c8b257bb99a3500e2c86a65400?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/868129c8b257bb99a3500e2c86a65400?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/abandlamudi"},"ccabreralomeli":{"type":"authors","id":"11708","meta":{"index":"authors_1591205172","id":"11708","found":true},"name":"Carlos Cabrera-Lomelí","firstName":"Carlos","lastName":"Cabrera-Lomelí","slug":"ccabreralomeli","email":"ccabreralomeli@KQED.org","display_author_email":true,"staff_mastheads":["news"],"title":"Community Reporter","bio":"Carlos Cabrera-Lomelí is a community reporter with KQED's digital engagement team. He also reports and co-produces for KQED's bilingual news hub KQED en Español. He grew up in San Francisco's Mission District and has previously worked with Univision, 48 Hills and REFORMA in Mexico City.","avatar":"https://secure.gravatar.com/avatar/e95ff80bb2eaf18a8f2af4dcf7ffb54b?s=600&d=blank&r=g","twitter":"@LomeliCabrera","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"arts","roles":["editor"]},{"site":"news","roles":["editor"]},{"site":"about","roles":["editor"]},{"site":"science","roles":["editor"]},{"site":"perspectives","roles":["editor"]},{"site":"elections","roles":["editor"]}],"headData":{"title":"Carlos Cabrera-Lomelí | KQED","description":"Community Reporter","ogImgSrc":"https://secure.gravatar.com/avatar/e95ff80bb2eaf18a8f2af4dcf7ffb54b?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/e95ff80bb2eaf18a8f2af4dcf7ffb54b?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/ccabreralomeli"},"amadrigal":{"type":"authors","id":"11757","meta":{"index":"authors_1591205172","id":"11757","found":true},"name":"Alexis Madrigal","firstName":"Alexis","lastName":"Madrigal","slug":"amadrigal","email":"amadrigal@kqed.org","display_author_email":true,"staff_mastheads":[],"title":"Co-Host Forum","bio":"Alexis Madrigal is the co-host of Forum. He is also a contributing writer at \u003cem>The Atlantic \u003c/em>and the co-founder of the COVID Tracking Project. He's the creator of the podcast, \u003cem>Containers\u003c/em>, and has been a staff writer at \u003cem>Wired. \u003c/em>He was a visiting scholar at UC Berkeley's Information School, and is working on a book about Oakland and the Bay Area's revolutionary ideas.","avatar":"https://secure.gravatar.com/avatar/200d13dd6cebef55bf04327dec901b3d?s=600&d=blank&r=g","twitter":"alexismadrigal","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"news","roles":["editor"]},{"site":"forum","roles":["editor"]}],"headData":{"title":"Alexis Madrigal | KQED","description":"Co-Host Forum","ogImgSrc":"https://secure.gravatar.com/avatar/200d13dd6cebef55bf04327dec901b3d?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/200d13dd6cebef55bf04327dec901b3d?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/amadrigal"},"daisynguyen":{"type":"authors","id":"11829","meta":{"index":"authors_1591205172","id":"11829","found":true},"name":"Daisy Nguyen","firstName":"Daisy","lastName":"Nguyen","slug":"daisynguyen","email":"daisynguyen@kqed.org","display_author_email":true,"staff_mastheads":["news"],"title":"KQED Contributor","bio":"Daisy Nguyen is KQED's early childhood education reporter. She focuses on the pandemic’s effect on young children; the child care crisis and its effects on families, caregivers and the economy; and how policy decisions affect individual lives and communities. Her work has appeared on NPR, Marketplace and Here & Now. She worked at The Associated Press for 20 years, covering breaking news throughout California.","avatar":"https://secure.gravatar.com/avatar/2da2127c27f7143b53ebd419800fd55f?s=600&d=blank&r=g","twitter":"@daisynguyen","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"news","roles":["author"]}],"headData":{"title":"Daisy Nguyen | KQED","description":"KQED Contributor","ogImgSrc":"https://secure.gravatar.com/avatar/2da2127c27f7143b53ebd419800fd55f?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/2da2127c27f7143b53ebd419800fd55f?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/daisynguyen"},"sjohnson":{"type":"authors","id":"11840","meta":{"index":"authors_1591205172","id":"11840","found":true},"name":"Sydney Johnson","firstName":"Sydney","lastName":"Johnson","slug":"sjohnson","email":"sjohnson@kqed.org","display_author_email":false,"staff_mastheads":["news"],"title":"KQED Reporter","bio":"Sydney Johnson is a general assignment reporter at KQED. She previously reported on public health and city government at the San Francisco Examiner, and before that, she covered statewide education policy for EdSource. Her reporting has won multiple local, state and national awards. Sydney is a graduate of the University of California, Berkeley and lives in San Francisco.","avatar":"https://secure.gravatar.com/avatar/97855f2719b72ad6190b7c535fe642c8?s=600&d=blank&r=g","twitter":"sydneyfjohnson","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"news","roles":["editor"]}],"headData":{"title":"Sydney Johnson | KQED","description":"KQED Reporter","ogImgSrc":"https://secure.gravatar.com/avatar/97855f2719b72ad6190b7c535fe642c8?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/97855f2719b72ad6190b7c535fe642c8?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/sjohnson"},"adembosky":{"type":"authors","id":"3205","meta":{"index":"authors_1591205172","id":"3205","found":true},"name":"April Dembosky","firstName":"April","lastName":"Dembosky","slug":"adembosky","email":"adembosky@kqed.org","display_author_email":false,"staff_mastheads":["news","science"],"title":"KQED Health Correspondent","bio":"April Dembosky is the health correspondent for KQED News and a regular contributor to NPR. She specializes in covering altered states of mind, from postpartum depression to methamphetamine-induced psychosis to the insanity defense. Her investigative series on insurance companies sidestepping mental health laws won multiple awards, including first place in beat reporting from the national Association of Health Care Journalists. She is the recipient of numerous other prizes and fellowships, including a national Edward R. Murrow award for investigative reporting, a Society of Professional Journalists award for long-form storytelling, and a Carter Center Fellowship for Mental Health Journalism.\r\n\r\nDembosky reported and produced \u003cem>Soundtrack of Silence\u003c/em>, an audio documentary about music and memory that is currently being made into a feature film by Paramount Pictures.\r\n\r\nBefore joining KQED in 2013, Dembosky covered technology and Silicon Valley for \u003cem>The Financial Times of London,\u003c/em> and contributed business and arts stories to \u003cem>Marketplace \u003c/em>and \u003cem>The New York Times.\u003c/em> She got her undergraduate degree in philosophy from Smith College and her master's in journalism from the University of California, Berkeley. She is a classically trained violinist and proud alum of the first symphony orchestra at Burning Man.","avatar":"https://secure.gravatar.com/avatar/ef92999be4ceb9ea60701e7dc276f813?s=600&d=blank&r=g","twitter":"adembosky","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"arts","roles":["author"]},{"site":"news","roles":["editor"]},{"site":"futureofyou","roles":["author"]},{"site":"stateofhealth","roles":["editor"]},{"site":"science","roles":["editor"]},{"site":"forum","roles":["editor"]}],"headData":{"title":"April Dembosky | KQED","description":"KQED Health Correspondent","ogImgSrc":"https://secure.gravatar.com/avatar/ef92999be4ceb9ea60701e7dc276f813?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/ef92999be4ceb9ea60701e7dc276f813?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/adembosky"}},"breakingNewsReducer":{},"campaignFinanceReducer":{},"firebase":{"requesting":{},"requested":{},"timestamps":{},"data":{},"ordered":{},"auth":{"isLoaded":false,"isEmpty":true},"authError":null,"profile":{"isLoaded":false,"isEmpty":true},"listeners":{"byId":{},"allIds":[]},"isInitializing":false,"errors":[]},"navBarReducer":{"navBarId":"news","fullView":true,"showPlayer":false},"navMenuReducer":{"menus":[{"key":"menu1","items":[{"name":"News","link":"/","type":"title"},{"name":"Politics","link":"/politics"},{"name":"Science","link":"/science"},{"name":"Education","link":"/educationnews"},{"name":"Housing","link":"/housing"},{"name":"Immigration","link":"/immigration"},{"name":"Criminal Justice","link":"/criminaljustice"},{"name":"Silicon Valley","link":"/siliconvalley"},{"name":"Forum","link":"/forum"},{"name":"The California Report","link":"/californiareport"}]},{"key":"menu2","items":[{"name":"Arts & Culture","link":"/arts","type":"title"},{"name":"Critics’ Picks","link":"/thedolist"},{"name":"Cultural Commentary","link":"/artscommentary"},{"name":"Food & Drink","link":"/food"},{"name":"Bay Area Hip-Hop","link":"/bayareahiphop"},{"name":"Rebel Girls","link":"/rebelgirls"},{"name":"Arts Video","link":"/artsvideos"}]},{"key":"menu3","items":[{"name":"Podcasts","link":"/podcasts","type":"title"},{"name":"Bay Curious","link":"/podcasts/baycurious"},{"name":"Rightnowish","link":"/podcasts/rightnowish"},{"name":"The Bay","link":"/podcasts/thebay"},{"name":"On Our Watch","link":"/podcasts/onourwatch"},{"name":"Mindshift","link":"/podcasts/mindshift"},{"name":"Consider This","link":"/podcasts/considerthis"},{"name":"Political Breakdown","link":"/podcasts/politicalbreakdown"}]},{"key":"menu4","items":[{"name":"Live Radio","link":"/radio","type":"title"},{"name":"TV","link":"/tv","type":"title"},{"name":"Events","link":"/events","type":"title"},{"name":"For Educators","link":"/education","type":"title"},{"name":"Support KQED","link":"/support","type":"title"},{"name":"About","link":"/about","type":"title"},{"name":"Help Center","link":"https://kqed-helpcenter.kqed.org/s","type":"title"}]}]},"pagesReducer":{},"postsReducer":{"stream_live":{"type":"live","id":"stream_live","audioUrl":"https://streams.kqed.org/kqedradio","title":"Live Stream","excerpt":"Live Stream information currently unavailable.","link":"/radio","featImg":"","label":{"name":"KQED Live","link":"/"}},"stream_kqedNewscast":{"type":"posts","id":"stream_kqedNewscast","audioUrl":"https://www.kqed.org/.stream/anon/radio/RDnews/newscast.mp3?_=1","title":"KQED Newscast","featImg":"","label":{"name":"88.5 FM","link":"/"}},"news_11983016":{"type":"posts","id":"news_11983016","meta":{"index":"posts_1591205157","site":"news","id":"11983016","found":true},"guestAuthors":[],"slug":"california-preschools-wrestle-to-comply-with-states-tightened-suspension-rules","title":"California Preschools Wrestle to Comply With State’s Tightened Suspension Rules","publishDate":1713265239,"format":"standard","headTitle":"California Preschools Wrestle to Comply With State’s Tightened Suspension Rules | KQED","labelTerm":{"term":72,"site":"news"},"content":"\u003cp>Like many babies born around the time of the COVID-19 shutdowns, 4-year-old Cole grew up watching \u003cem>Cocomelon\u003c/em> and \u003cem>Bluey\u003c/em>.\u003c/p>\n\u003cp>The popular kids shows kept him entertained while his mom, Grace McPherson, helped his older sister with distance learning. However, too much screen time and social isolation took a toll on Cole’s development. His mom said he was “pretty much nonverbal” when he was 3 years old.[pullquote size=\"medium\" align=\"right\" citation=\"Grace McPherson, mother of 4-year-old Cole\"]‘They said that he’s not ready for preschool, and I was just shocked.’[/pullquote]So last fall, McPherson enrolled her son in a preschool in the Bay Area town of Oakley to help him catch up. The first day went smoothly. But on the second day, not long after dropping him off, the school called McPherson to pick up Cole because he refused to sit at circle time and was crying inconsolably.\u003c/p>\n\u003cp>“They said that he’s not ready for preschool, and I was just shocked,” she said.\u003c/p>\n\u003cp>The preschool director suggested coming back when Cole was more ready to follow directions, McPherson said. But she had made up her mind: she’d rather forfeit the $400 deposit for his tuition than return to a preschool that couldn’t support her son through a tantrum.\u003c/p>\n\u003cp>“I felt like they were just passing the buck,” she said. “And it’s just, ‘Here you go, here’s your child back. Figure out something else.’”\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>The school never told McPherson they suspended her son when they asked her to take him home. Still, their experience would be considered a suspension under a state law designed to limit exclusionary discipline in early childhood education.[pullquote size=\"medium\" align=\"right\" citation=\"Nina Buthee, executive director, EveryChild California\"]‘The intention is good, but in actuality, there just aren’t the resources there to help support these preschool programs to do it in a really effective way.’[/pullquote]Suspending or expelling children from preschool for hitting, biting and other challenging behavior\u003ca href=\"https://cep.asu.edu/sites/default/files/2022-09/exclusionary-discipline-093022-1.pdf\"> is surprisingly common\u003c/a>. It happens way more often to Black children, boys, and children with learning differences than others, according to the most recent \u003ca href=\"https://www2.ed.gov/about/offices/list/ocr/docs/crdc-discipline-school-climate-report.pdf\">federal civil rights data. \u003c/a>\u003c/p>\n\u003cp>California recently toughened rules around exclusionary discipline at preschools and child care centers that receive state funding, but implementing them has been tough for providers who are still dealing with stressed-out teachers, kids with fewer social skills and other long-lasting effects of the pandemic.\u003c/p>\n\u003cp>“The intention is good, but in actuality, there just aren’t the resources there to help support these preschool programs to do it in a really effective way,” said Nina Buthee, executive director of EveryChild California, an association of publicly funded early education programs.\u003c/p>\n\u003ch2>‘What it means to exclude a child’\u003c/h2>\n\u003cp>California is among 24 states with laws limiting preschool suspension and expulsion, according to \u003ca href=\"https://cep.asu.edu/sites/default/files/2023-12/state-discipline-120523_0.pdf\">the Children’s Equity Project\u003c/a> at Arizona State University, because studies have found that children who are removed from their classroom or sent home from school as a form of discipline tend to repeat the pattern in later years and become disengaged from school.\u003c/p>\n\u003cp>“It’s not acceptable,” said Adonai Mack, a founding member of Black Men for Education Equity, which advocated for the law. “There should be no reason why a young child in their earliest development is excluded from an educational opportunity.”\u003c/p>\n\u003cfigure id=\"attachment_11976825\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11976825\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED.jpg\" alt=\"\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003cfigcaption class=\"wp-caption-text\">Grace McPherson spends time with her son Cole, 3, at Los Medanos College Child Study Center in Pittsburg on Feb. 15, 2024. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>A 2017 law requires state-funded preschools to pursue and document ways they tried to support children with challenging behavior before resorting to expulsion. Another law passed in 2022 prohibits expulsion \u003cem>and\u003c/em> suspension and applies to both preschools and state-subsidized child care programs for infants and toddlers.[pullquote size=\"medium\" align=\"right\" citation=\"Adonai Mack, founding member, Black Men for Education Equity\"]‘There should be no reason why a young child in their earliest development is excluded from an educational opportunity.’[/pullquote]\u003ca href=\"https://www.cde.ca.gov/sp/cd/ci/mb2308.asp\">The rules \u003c/a>specifically prohibit teachers from sending children to another room or home in the middle of the day because of their behavior. That would be considered suspension. Teachers also can’t encourage a parent to unenroll from a program, and suspension or expulsion can only be used as a last resort when serious safety concerns exist.\u003c/p>\n\u003cp>The California law outlines one of the clearest definitions of suspension and expulsion, said Walter Gilliam, executive director of the Buffett Early Childhood Institute at the University of Nebraska.\u003c/p>\n\u003cp>Gilliam said teachers often don’t realize they’re suspending or expelling a child when they advise parents to find another school that’s “a better fit” or when they repeatedly ask parents to pick up their child early, creating an inconvenience that could lead parents to look elsewhere for more reliable child care.\u003c/p>\n\u003cp>“When we’re not very clear about what it means to exclude a child, then we run the risk of local implementers thinking that an exclusion means one thing and policymakers thinking that it means a completely different thing,” he said.\u003c/p>\n\u003cfigure id=\"attachment_11976829\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11976829\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED.jpg\" alt=\"\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003cfigcaption class=\"wp-caption-text\">Danielle Jorgenson, known to students as Teacher Dani, cheers for students as they jump during a preschool class at Los Medanos College Child Study Center in Pittsburg on Feb. 15, 2024. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>To ensure accountability, California law requires teachers to document ways they try to support children with challenging behaviors, such as setting behavior goals along with their parents and referring them to mental health consultants. Parents have the right to appeal a suspension or expulsion to state authorities.\u003c/p>\n\u003cp>To help make the policy work, lawmakers increased funding for preschool and child care centers that provide early childhood mental health consultation services — such as marriage and family therapists, social workers and child psychologists — for kids, their families or teachers.[aside postID=news_11979071 hero='https://cdn.kqed.org/wp-content/uploads/sites/10/2024/03/240309-EARLY-START-DEVELOPMENTAL-DELAYS-MD-02-KQED-1-1020x680.jpg']But Buthee said the law is placing demands on preschools and child care centers that are stretched thin by staffing shortages. Teachers sometimes get caught between providing one-on-one support for an ill-behaved child and ensuring there are enough adults in the room for the rest of the class.\u003c/p>\n\u003cp>Requiring teachers to keep records of how they dealt with a child acting up “feels like a gotcha policy” and makes a bigger deal out of what might be an age-appropriate behavior.\u003c/p>\n\u003cp>Members are also telling her they have a hard time finding early childhood mental health consultants.\u003c/p>\n\u003cp>“To actually find an individual in their community who is able to come in for an hour or a couple hours a week on a pretty short-term basis is very challenging,” she said.\u003c/p>\n\u003ch2>Building trust in a child’s life\u003c/h2>\n\u003cp>Linda Brault with the education research organization WestEd has seen this, too. She trains preschool teachers to work with children with challenging behavior.\u003c/p>\n\u003cp>“Right now, the stress level of the provider, and the fact that so many people haven’t gotten time to go to a training because they don’t have substitutes, or they’re working two jobs or whatever … I think we really have to address that,” she said.\u003c/p>\n\u003cfigure id=\"attachment_11976828\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11976828\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED.jpg\" alt=\"\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003cfigcaption class=\"wp-caption-text\">Danielle Jorgenson, known to students as Teacher Dani, works with Cole, 3, in the garden during a preschool class at Los Medanos College Child Study Center in Pittsburg on Feb. 15, 2024. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>The issue is crucial because the more stressed a teacher is, the more likely the teacher is to discipline a child. When teachers do have enough professional support and training to respond to a misbehaving child, Brault said, they tend to stay in their job and have fewer problems in the classroom.\u003c/p>\n\u003cp>“There is documentation and data that says children who are expelled and suspended in early childhood have a tendency to continue that pattern, so we really want to interrupt that,” she said.\u003c/p>\n\u003cp>McPherson eventually enrolled her son Cole at the Child Study Center, a preschool on the campus of Los Medanos College in Pittsburg, which is also a training ground for early educators. For the last decade, the school has been working hard to prevent suspensions and expulsions by meeting children where they’re at emotionally and developmentally.[aside postID=news_11968835 hero='https://ww2.kqed.org/app/uploads/sites/10/2023/12/20231108-Alameda-Black-Maternal-Health-021-JY-qut-1020x680.jpg']Cole’s teacher Danielle Jorgensen said when he first got there, he had trouble communicating.\u003c/p>\n\u003cp>“He would try to tell us something. We couldn’t understand him. So he would fall to the ground, kick and scream,” she said.\u003c/p>\n\u003cp>She said she would get on the floor, take deep breaths and try to understand him. If you discipline a child while their brain is not able to think and process, she said, you’re not helping the child learn how to self-calm.\u003c/p>\n\u003cp>“A lot of the things that we work on here is teaching them that it’s OK to have emotions and how to deal with them,” she said.\u003c/p>\n\u003cp>Jorgensen can take the time to work individually with Cole because there were enough interns in the room to watch over the other children, thanks to the preschool’s unique relationship with the college. She said she also tries to build relationships with parents and their kids to foster trust because once children feel safe, their brains are more open to learning.[pullquote size=\"medium\" align=\"right\" citation=\"Grace McPherson, mother to 4-year-old Cole\"]‘It really starts with the attuned, calm, trusted caregiver, teacher, parent in the child’s life. That really sets the tone for the relationships that the kids are going to have.’[/pullquote]McPherson said in just a few months, her son’s vocabulary exploded.\u003c/p>\n\u003cp>“His confidence, his ability to make friends, just overall his growth was extraordinary,” she said.\u003c/p>\n\u003cp>Getting her son reliable child care allowed McPherson to go back to school. She enrolled at Los Medanos to get a certification to teach middle school. She also received a grant to lower Cole’s preschool tuition, and in turn, she had to take a child development class and volunteer as a helper at the preschool.\u003c/p>\n\u003cp>She said the class gave her a greater appreciation for conscious discipline, a series of strategies used at the Child Study Center to teach social-emotional skills.\u003c/p>\n\u003cp>“It really starts with the attuned, calm, trusted caregiver, teacher, parent in the child’s life. That really sets the tone for the relationships that the kids are going to have,” she said.\u003c/p>\n\u003cp>\u003cem>For more information about California’s laws and how to prevent suspension and expulsion in early child care and education programs, check out \u003c/em>\u003ca href=\"https://preventingchildcareexpulsionca.org/\">\u003cem>https://preventingchildcareexpulsionca.org/\u003c/em>\u003c/a>\u003cem>.\u003c/em>\u003c/p>\n\u003cp>[ad floatright]\u003c/p>\n","blocks":[],"excerpt":" New state rules make it harder for child care and preschool programs that receive state funding to suspend or expel children. Providers say the rules are placing more demands on a workforce still coping with post-pandemic challenges. ","status":"publish","parent":0,"modified":1713283405,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":35,"wordCount":1882},"headData":{"title":"California Preschools Wrestle to Comply With State’s Tightened Suspension Rules | KQED","description":" New state rules make it harder for child care and preschool programs that receive state funding to suspend or expel children. Providers say the rules are placing more demands on a workforce still coping with post-pandemic challenges. ","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"audioUrl":"https://traffic.omny.fm/d/clips/0af137ef-751e-4b19-a055-aaef00d2d578/ffca7e9f-6831-41c5-bcaf-aaef00f5a073/0899d87b-9cb1-4efd-9a9c-b15301009962/audio.mp3","sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/news/11983016/california-preschools-wrestle-to-comply-with-states-tightened-suspension-rules","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>Like many babies born around the time of the COVID-19 shutdowns, 4-year-old Cole grew up watching \u003cem>Cocomelon\u003c/em> and \u003cem>Bluey\u003c/em>.\u003c/p>\n\u003cp>The popular kids shows kept him entertained while his mom, Grace McPherson, helped his older sister with distance learning. However, too much screen time and social isolation took a toll on Cole’s development. His mom said he was “pretty much nonverbal” when he was 3 years old.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘They said that he’s not ready for preschool, and I was just shocked.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Grace McPherson, mother of 4-year-old Cole","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>So last fall, McPherson enrolled her son in a preschool in the Bay Area town of Oakley to help him catch up. The first day went smoothly. But on the second day, not long after dropping him off, the school called McPherson to pick up Cole because he refused to sit at circle time and was crying inconsolably.\u003c/p>\n\u003cp>“They said that he’s not ready for preschool, and I was just shocked,” she said.\u003c/p>\n\u003cp>The preschool director suggested coming back when Cole was more ready to follow directions, McPherson said. But she had made up her mind: she’d rather forfeit the $400 deposit for his tuition than return to a preschool that couldn’t support her son through a tantrum.\u003c/p>\n\u003cp>“I felt like they were just passing the buck,” she said. “And it’s just, ‘Here you go, here’s your child back. Figure out something else.’”\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>The school never told McPherson they suspended her son when they asked her to take him home. Still, their experience would be considered a suspension under a state law designed to limit exclusionary discipline in early childhood education.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘The intention is good, but in actuality, there just aren’t the resources there to help support these preschool programs to do it in a really effective way.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Nina Buthee, executive director, EveryChild California","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>Suspending or expelling children from preschool for hitting, biting and other challenging behavior\u003ca href=\"https://cep.asu.edu/sites/default/files/2022-09/exclusionary-discipline-093022-1.pdf\"> is surprisingly common\u003c/a>. It happens way more often to Black children, boys, and children with learning differences than others, according to the most recent \u003ca href=\"https://www2.ed.gov/about/offices/list/ocr/docs/crdc-discipline-school-climate-report.pdf\">federal civil rights data. \u003c/a>\u003c/p>\n\u003cp>California recently toughened rules around exclusionary discipline at preschools and child care centers that receive state funding, but implementing them has been tough for providers who are still dealing with stressed-out teachers, kids with fewer social skills and other long-lasting effects of the pandemic.\u003c/p>\n\u003cp>“The intention is good, but in actuality, there just aren’t the resources there to help support these preschool programs to do it in a really effective way,” said Nina Buthee, executive director of EveryChild California, an association of publicly funded early education programs.\u003c/p>\n\u003ch2>‘What it means to exclude a child’\u003c/h2>\n\u003cp>California is among 24 states with laws limiting preschool suspension and expulsion, according to \u003ca href=\"https://cep.asu.edu/sites/default/files/2023-12/state-discipline-120523_0.pdf\">the Children’s Equity Project\u003c/a> at Arizona State University, because studies have found that children who are removed from their classroom or sent home from school as a form of discipline tend to repeat the pattern in later years and become disengaged from school.\u003c/p>\n\u003cp>“It’s not acceptable,” said Adonai Mack, a founding member of Black Men for Education Equity, which advocated for the law. “There should be no reason why a young child in their earliest development is excluded from an educational opportunity.”\u003c/p>\n\u003cfigure id=\"attachment_11976825\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11976825\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED.jpg\" alt=\"\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-14-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003cfigcaption class=\"wp-caption-text\">Grace McPherson spends time with her son Cole, 3, at Los Medanos College Child Study Center in Pittsburg on Feb. 15, 2024. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>A 2017 law requires state-funded preschools to pursue and document ways they tried to support children with challenging behavior before resorting to expulsion. Another law passed in 2022 prohibits expulsion \u003cem>and\u003c/em> suspension and applies to both preschools and state-subsidized child care programs for infants and toddlers.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘There should be no reason why a young child in their earliest development is excluded from an educational opportunity.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Adonai Mack, founding member, Black Men for Education Equity","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003ca href=\"https://www.cde.ca.gov/sp/cd/ci/mb2308.asp\">The rules \u003c/a>specifically prohibit teachers from sending children to another room or home in the middle of the day because of their behavior. That would be considered suspension. Teachers also can’t encourage a parent to unenroll from a program, and suspension or expulsion can only be used as a last resort when serious safety concerns exist.\u003c/p>\n\u003cp>The California law outlines one of the clearest definitions of suspension and expulsion, said Walter Gilliam, executive director of the Buffett Early Childhood Institute at the University of Nebraska.\u003c/p>\n\u003cp>Gilliam said teachers often don’t realize they’re suspending or expelling a child when they advise parents to find another school that’s “a better fit” or when they repeatedly ask parents to pick up their child early, creating an inconvenience that could lead parents to look elsewhere for more reliable child care.\u003c/p>\n\u003cp>“When we’re not very clear about what it means to exclude a child, then we run the risk of local implementers thinking that an exclusion means one thing and policymakers thinking that it means a completely different thing,” he said.\u003c/p>\n\u003cfigure id=\"attachment_11976829\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11976829\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED.jpg\" alt=\"\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-35-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003cfigcaption class=\"wp-caption-text\">Danielle Jorgenson, known to students as Teacher Dani, cheers for students as they jump during a preschool class at Los Medanos College Child Study Center in Pittsburg on Feb. 15, 2024. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>To ensure accountability, California law requires teachers to document ways they try to support children with challenging behaviors, such as setting behavior goals along with their parents and referring them to mental health consultants. Parents have the right to appeal a suspension or expulsion to state authorities.\u003c/p>\n\u003cp>To help make the policy work, lawmakers increased funding for preschool and child care centers that provide early childhood mental health consultation services — such as marriage and family therapists, social workers and child psychologists — for kids, their families or teachers.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11979071","hero":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/03/240309-EARLY-START-DEVELOPMENTAL-DELAYS-MD-02-KQED-1-1020x680.jpg","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>But Buthee said the law is placing demands on preschools and child care centers that are stretched thin by staffing shortages. Teachers sometimes get caught between providing one-on-one support for an ill-behaved child and ensuring there are enough adults in the room for the rest of the class.\u003c/p>\n\u003cp>Requiring teachers to keep records of how they dealt with a child acting up “feels like a gotcha policy” and makes a bigger deal out of what might be an age-appropriate behavior.\u003c/p>\n\u003cp>Members are also telling her they have a hard time finding early childhood mental health consultants.\u003c/p>\n\u003cp>“To actually find an individual in their community who is able to come in for an hour or a couple hours a week on a pretty short-term basis is very challenging,” she said.\u003c/p>\n\u003ch2>Building trust in a child’s life\u003c/h2>\n\u003cp>Linda Brault with the education research organization WestEd has seen this, too. She trains preschool teachers to work with children with challenging behavior.\u003c/p>\n\u003cp>“Right now, the stress level of the provider, and the fact that so many people haven’t gotten time to go to a training because they don’t have substitutes, or they’re working two jobs or whatever … I think we really have to address that,” she said.\u003c/p>\n\u003cfigure id=\"attachment_11976828\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11976828\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED.jpg\" alt=\"\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/240215-PRESCHOOLSUSPENSION-29-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003cfigcaption class=\"wp-caption-text\">Danielle Jorgenson, known to students as Teacher Dani, works with Cole, 3, in the garden during a preschool class at Los Medanos College Child Study Center in Pittsburg on Feb. 15, 2024. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>The issue is crucial because the more stressed a teacher is, the more likely the teacher is to discipline a child. When teachers do have enough professional support and training to respond to a misbehaving child, Brault said, they tend to stay in their job and have fewer problems in the classroom.\u003c/p>\n\u003cp>“There is documentation and data that says children who are expelled and suspended in early childhood have a tendency to continue that pattern, so we really want to interrupt that,” she said.\u003c/p>\n\u003cp>McPherson eventually enrolled her son Cole at the Child Study Center, a preschool on the campus of Los Medanos College in Pittsburg, which is also a training ground for early educators. For the last decade, the school has been working hard to prevent suspensions and expulsions by meeting children where they’re at emotionally and developmentally.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11968835","hero":"https://ww2.kqed.org/app/uploads/sites/10/2023/12/20231108-Alameda-Black-Maternal-Health-021-JY-qut-1020x680.jpg","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>Cole’s teacher Danielle Jorgensen said when he first got there, he had trouble communicating.\u003c/p>\n\u003cp>“He would try to tell us something. We couldn’t understand him. So he would fall to the ground, kick and scream,” she said.\u003c/p>\n\u003cp>She said she would get on the floor, take deep breaths and try to understand him. If you discipline a child while their brain is not able to think and process, she said, you’re not helping the child learn how to self-calm.\u003c/p>\n\u003cp>“A lot of the things that we work on here is teaching them that it’s OK to have emotions and how to deal with them,” she said.\u003c/p>\n\u003cp>Jorgensen can take the time to work individually with Cole because there were enough interns in the room to watch over the other children, thanks to the preschool’s unique relationship with the college. She said she also tries to build relationships with parents and their kids to foster trust because once children feel safe, their brains are more open to learning.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘It really starts with the attuned, calm, trusted caregiver, teacher, parent in the child’s life. That really sets the tone for the relationships that the kids are going to have.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Grace McPherson, mother to 4-year-old Cole","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>McPherson said in just a few months, her son’s vocabulary exploded.\u003c/p>\n\u003cp>“His confidence, his ability to make friends, just overall his growth was extraordinary,” she said.\u003c/p>\n\u003cp>Getting her son reliable child care allowed McPherson to go back to school. She enrolled at Los Medanos to get a certification to teach middle school. She also received a grant to lower Cole’s preschool tuition, and in turn, she had to take a child development class and volunteer as a helper at the preschool.\u003c/p>\n\u003cp>She said the class gave her a greater appreciation for conscious discipline, a series of strategies used at the Child Study Center to teach social-emotional skills.\u003c/p>\n\u003cp>“It really starts with the attuned, calm, trusted caregiver, teacher, parent in the child’s life. That really sets the tone for the relationships that the kids are going to have,” she said.\u003c/p>\n\u003cp>\u003cem>For more information about California’s laws and how to prevent suspension and expulsion in early child care and education programs, check out \u003c/em>\u003ca href=\"https://preventingchildcareexpulsionca.org/\">\u003cem>https://preventingchildcareexpulsionca.org/\u003c/em>\u003c/a>\u003cem>.\u003c/em>\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"floatright"},"numeric":["floatright"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983016/california-preschools-wrestle-to-comply-with-states-tightened-suspension-rules","authors":["11829"],"programs":["news_72"],"categories":["news_8"],"tags":["news_22570","news_32102","news_20013","news_27626","news_17763"],"featImg":"news_11976827","label":"news_72"},"news_11983146":{"type":"posts","id":"news_11983146","meta":{"index":"posts_1591205157","site":"news","id":"11983146","found":true},"guestAuthors":[],"slug":"san-franciscos-new-parking-rules-set-to-displace-rv-community-near-sf-state","title":"San Francisco’s New Parking Rules Set to Displace RV Community Near SF State","publishDate":1713306661,"format":"standard","headTitle":"San Francisco’s New Parking Rules Set to Displace RV Community Near SF State | KQED","labelTerm":{"site":"news"},"content":"\u003cp>After months of pressure from advocates to \u003ca href=\"https://www.kqed.org/news/11970299/city-delays-parking-restrictions-near-sf-state-offering-brief-reprieve-to-rv-community\">delay parking enforcement\u003c/a>, San Francisco will begin requiring vehicles to be moved every four hours on streets between SF State and Stonestown Galleria, affecting a large RV community in the area.\u003c/p>\n\u003cp>[pullquote size=\"medium\" align=\"right\" citation=\"Yessica Hernandez, organizer\"]‘You say this is for the safety for the public. But where are these people going to go after they are displaced? We aren’t thinking about that.’[/pullquote]Clusters of mobile homes have popped up around the Bay Area as housing has grown out of reach for many. However, the city’s effort to \u003ca href=\"https://www.kqed.org/news/11965352/san-francisco-rv-community-fears-new-parking-rules-could-push-them-closer-to-homelessness\">evict RVs through parking restrictions\u003c/a> has been met with controversy. While some residents say mobile vehicles clutter their sidewalks and present safety issues, others say the RVs are homes and urge the city to find a long-term solution where they can park.\u003c/p>\n\u003cp>Marlon Arostegui has lived in an RV in the neighborhood for two years.[aside postID=\"news_11965352,news_11970299,news_11979919\" label=\"Related Stories\"]He has a job in towing to support his niece and her partner and said he doesn’t yet know what he will do when the parking tickets start.\u003c/p>\n\u003cp>“I’ve been living at Winston Drive, and we’ve been informed that we will get parking restrictions,” Arostegui said through a Spanish translator during the San Francisco Municipal Transportation Agency’s board meeting. “We’re asking for your support in finding a secure place to park.”\u003c/p>\n\u003cp>The new rules limit parking to four hours between Lake Merced Boulevard and Buckingham Way from 8 a.m. to 6 p.m. Monday to Friday.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>The city has not stated exactly when the new parking restrictions will begin, but new parking limit signs are now erected. Residents living in RVs in the area were given a paper flier saying that “enforcement will begin soon” for the four-hour time limits.\u003c/p>\n\u003cp>“We don’t have the conditions to pay for rent,” Leticia, who lives in an RV with her two children on Winston Drive, said at Tuesday’s SFMTA meeting. “We need a safe place. We don’t have anywhere else to go. My two daughters are in school, and I need a safe place for both of them.”\u003c/p>\n\u003cfigure id=\"attachment_11983160\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11983160\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED.jpg\" alt=\"A man wearing a black and white track suit stands next to a woman with a green shirt in front of microphones inside a building.\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">Marlon Arostegui speaks at an SFMTA Board of Directors meeting at San Francisco City Hall on April 16, 2024. \u003ccite>(Martin do Nascimento/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>During Tuesday’s SFMTA board meeting, Director Jeffrey Tumlin said, however, that the city “will not be doing any enforcement of these new signs” until after a nearby road paving program is complete and after the Department of Homelessness and Supportive Housing can do additional rounds of outreach to RV residents.\u003c/p>\n\u003cp>Parking and traffic safety enforcement will ramp up across the entire city in the coming weeks as the city has hired more parking patrol officers, Tumlin said.\u003c/p>\n\u003cp>Several speakers on Tuesday protested the decision and said that they couldn’t move their vehicles because they were at work during the day. Others needed help repairing a mechanical issue in order to drive.\u003c/p>\n\u003cp>Many said they wouldn’t be able to pay the $92 ticket that the city would issue to cars that don’t move and fear those tickets could further entrench their housing challenges.\u003c/p>\n\u003cfigure id=\"attachment_11983159\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11983159\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED.jpg\" alt=\"Three women and one man sit behind a table with microphones and computer screens.\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">SFMTA Board Chair Amanda Eaken (center right) and others listen to public comments during an SFMTA Board of Directors meeting at San Francisco City Hall on April 16, 2024. \u003ccite>(Martin do Nascimento/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>Across San Francisco, people living in RVs are in similar face offs with the city. About 35 RV dwellers were facing displacement when the city announced it would begin enforcing parking limits near Bernal Heights Park.\u003c/p>\n\u003cp>Some neighbors complained the vehicles clogged up the road and sidewalk around the park. But a \u003ca href=\"https://missionlocal.org/2024/03/bernal-heights-residents-buck-trend-and-fight-rv-evictions/\">group of housed neighbors\u003c/a> has also come together to delay enforcement until residents have an alternative place to go.\u003c/p>\n\u003cp>San Francisco’s Department of Homelessness and Supportive Housing has been working with people living in RVs on Winston Ave. for months to find housing placements and other solutions for people who want to stay in their RVs.\u003c/p>\n\u003cp>The Department previously told KQED it was reviewing potential locations where people living on Winstron could safely park their RVs. But no such location has been identified.\u003c/p>\n\u003cfigure id=\"attachment_11965074\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11965074\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED.jpg\" alt=\"A ticket on a windshield of a vehicle.\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">An SFMTA parking ticket for street cleaning sits on the windshield of an RV along Winston Drive in San Francisco, California, on Oct. 17, 2023, near San Francisco State University. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>“You’ll be displacing a lot of families. You say this is for the safety for the public. But where are these people going to go after they are displaced? We aren’t thinking about that,” Yessica Hernandez, an organizer who has been working with families living on Winston Drive, said during public comment. “We have a huge problem with homelessness in San Francisco, and we aren’t going to get rid of it by putting in four-hour parking restrictions.”\u003c/p>\n\u003cp>As of Tuesday, many residents who came to speak at City Hall said they felt stranded without many options ahead.\u003c/p>\n\u003cp>\u003c/p>\n\u003cp>“We need from you a safe place where we can move,” Walter Mejia, who has lived in an RV on Winston Dr for three years, said through a Spanish translator during Tuesday’s board meeting. “We don’t have the funds to pay for these parking tickets.”\u003c/p>\n\n","blocks":[],"excerpt":"Housed residents say mobile vehicles clutter their sidewalks, but RV dwellers say it’s home and there’s nowhere else to park. ","status":"publish","parent":0,"modified":1713307581,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":20,"wordCount":934},"headData":{"title":"San Francisco’s New Parking Rules Set to Displace RV Community Near SF State | KQED","description":"Housed residents say mobile vehicles clutter their sidewalks, but RV dwellers say it’s home and there’s nowhere else to park. ","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/news/11983146/san-franciscos-new-parking-rules-set-to-displace-rv-community-near-sf-state","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>After months of pressure from advocates to \u003ca href=\"https://www.kqed.org/news/11970299/city-delays-parking-restrictions-near-sf-state-offering-brief-reprieve-to-rv-community\">delay parking enforcement\u003c/a>, San Francisco will begin requiring vehicles to be moved every four hours on streets between SF State and Stonestown Galleria, affecting a large RV community in the area.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘You say this is for the safety for the public. But where are these people going to go after they are displaced? We aren’t thinking about that.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Yessica Hernandez, organizer","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>Clusters of mobile homes have popped up around the Bay Area as housing has grown out of reach for many. However, the city’s effort to \u003ca href=\"https://www.kqed.org/news/11965352/san-francisco-rv-community-fears-new-parking-rules-could-push-them-closer-to-homelessness\">evict RVs through parking restrictions\u003c/a> has been met with controversy. While some residents say mobile vehicles clutter their sidewalks and present safety issues, others say the RVs are homes and urge the city to find a long-term solution where they can park.\u003c/p>\n\u003cp>Marlon Arostegui has lived in an RV in the neighborhood for two years.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11965352,news_11970299,news_11979919","label":"Related Stories "},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>He has a job in towing to support his niece and her partner and said he doesn’t yet know what he will do when the parking tickets start.\u003c/p>\n\u003cp>“I’ve been living at Winston Drive, and we’ve been informed that we will get parking restrictions,” Arostegui said through a Spanish translator during the San Francisco Municipal Transportation Agency’s board meeting. “We’re asking for your support in finding a secure place to park.”\u003c/p>\n\u003cp>The new rules limit parking to four hours between Lake Merced Boulevard and Buckingham Way from 8 a.m. to 6 p.m. Monday to Friday.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>The city has not stated exactly when the new parking restrictions will begin, but new parking limit signs are now erected. Residents living in RVs in the area were given a paper flier saying that “enforcement will begin soon” for the four-hour time limits.\u003c/p>\n\u003cp>“We don’t have the conditions to pay for rent,” Leticia, who lives in an RV with her two children on Winston Drive, said at Tuesday’s SFMTA meeting. “We need a safe place. We don’t have anywhere else to go. My two daughters are in school, and I need a safe place for both of them.”\u003c/p>\n\u003cfigure id=\"attachment_11983160\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11983160\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED.jpg\" alt=\"A man wearing a black and white track suit stands next to a woman with a green shirt in front of microphones inside a building.\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-02-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">Marlon Arostegui speaks at an SFMTA Board of Directors meeting at San Francisco City Hall on April 16, 2024. \u003ccite>(Martin do Nascimento/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>During Tuesday’s SFMTA board meeting, Director Jeffrey Tumlin said, however, that the city “will not be doing any enforcement of these new signs” until after a nearby road paving program is complete and after the Department of Homelessness and Supportive Housing can do additional rounds of outreach to RV residents.\u003c/p>\n\u003cp>Parking and traffic safety enforcement will ramp up across the entire city in the coming weeks as the city has hired more parking patrol officers, Tumlin said.\u003c/p>\n\u003cp>Several speakers on Tuesday protested the decision and said that they couldn’t move their vehicles because they were at work during the day. Others needed help repairing a mechanical issue in order to drive.\u003c/p>\n\u003cp>Many said they wouldn’t be able to pay the $92 ticket that the city would issue to cars that don’t move and fear those tickets could further entrench their housing challenges.\u003c/p>\n\u003cfigure id=\"attachment_11983159\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11983159\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED.jpg\" alt=\"Three women and one man sit behind a table with microphones and computer screens.\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240415-RV-COMMUNITY-RALLY-MD-01-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">SFMTA Board Chair Amanda Eaken (center right) and others listen to public comments during an SFMTA Board of Directors meeting at San Francisco City Hall on April 16, 2024. \u003ccite>(Martin do Nascimento/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>Across San Francisco, people living in RVs are in similar face offs with the city. About 35 RV dwellers were facing displacement when the city announced it would begin enforcing parking limits near Bernal Heights Park.\u003c/p>\n\u003cp>Some neighbors complained the vehicles clogged up the road and sidewalk around the park. But a \u003ca href=\"https://missionlocal.org/2024/03/bernal-heights-residents-buck-trend-and-fight-rv-evictions/\">group of housed neighbors\u003c/a> has also come together to delay enforcement until residents have an alternative place to go.\u003c/p>\n\u003cp>San Francisco’s Department of Homelessness and Supportive Housing has been working with people living in RVs on Winston Ave. for months to find housing placements and other solutions for people who want to stay in their RVs.\u003c/p>\n\u003cp>The Department previously told KQED it was reviewing potential locations where people living on Winstron could safely park their RVs. But no such location has been identified.\u003c/p>\n\u003cfigure id=\"attachment_11965074\" class=\"wp-caption aligncenter\" style=\"max-width: 2000px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11965074\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED.jpg\" alt=\"A ticket on a windshield of a vehicle.\" width=\"2000\" height=\"1333\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED.jpg 2000w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-800x533.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-1020x680.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-160x107.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-1536x1024.jpg 1536w, https://cdn.kqed.org/wp-content/uploads/sites/10/2023/10/231017-LakeMercedRVs-023-BL-KQED-1920x1280.jpg 1920w\" sizes=\"(max-width: 2000px) 100vw, 2000px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">An SFMTA parking ticket for street cleaning sits on the windshield of an RV along Winston Drive in San Francisco, California, on Oct. 17, 2023, near San Francisco State University. \u003ccite>(Beth LaBerge/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>“You’ll be displacing a lot of families. You say this is for the safety for the public. But where are these people going to go after they are displaced? We aren’t thinking about that,” Yessica Hernandez, an organizer who has been working with families living on Winston Drive, said during public comment. “We have a huge problem with homelessness in San Francisco, and we aren’t going to get rid of it by putting in four-hour parking restrictions.”\u003c/p>\n\u003cp>As of Tuesday, many residents who came to speak at City Hall said they felt stranded without many options ahead.\u003c/p>\n\u003cp>\u003c/p>\n\u003cp>“We need from you a safe place where we can move,” Walter Mejia, who has lived in an RV on Winston Dr for three years, said through a Spanish translator during Tuesday’s board meeting. “We don’t have the funds to pay for these parking tickets.”\u003c/p>\n\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983146/san-franciscos-new-parking-rules-set-to-displace-rv-community-near-sf-state","authors":["11840"],"categories":["news_8"],"tags":["news_27626","news_25314","news_24635","news_31793"],"featImg":"news_11965073","label":"news"},"news_11983120":{"type":"posts","id":"news_11983120","meta":{"index":"posts_1591205157","site":"news","id":"11983120","found":true},"guestAuthors":[],"slug":"a-new-bay-area-clasico-sfs-el-farolito-and-oakland-roots-set-to-battle-in-hayward","title":"A New Bay Area Clásico? SF's El Farolito and Oakland Roots Set to Battle in Hayward","publishDate":1713301252,"format":"standard","headTitle":"A New Bay Area Clásico? SF’s El Farolito and Oakland Roots Set to Battle in Hayward | KQED","labelTerm":{"site":"news"},"content":"\u003cp>Two Bay Area teams — one hailing from San Francisco and the other representing Oakland — face off on Tuesday.\u003c/p>\n\u003cp>Both teams boast storied histories and steadfast fans. But this isn’t the Giants and A’s we’re talking about, but rather \u003ca href=\"https://www.ussoccer.com/us-open-cup/watch?matchId=cd399be4-9cc2-4806-aeb9-dd2ae5b927e7\">San Francisco’s El Farolito soccer team vs. Oakland Roots Soccer Club\u003c/a>.\u003c/p>\n\u003cp>This crucial match, kicking off at Cal State East Bay’s Pioneer Stadium in Hayward at 7:30 p.m. on Tuesday, marks the third round of the \u003ca href=\"https://www.ussoccer.com/us-open-cup/\">U.S. Open Cup\u003c/a> — the oldest soccer competition in the country that brings teams together that usually play in different leagues.\u003c/p>\n\u003cp>\u003cem>Stream the game \u003ca href=\"https://www.ussoccer.com/us-open-cup/watch?matchId=cd399be4-9cc2-4806-aeb9-dd2ae5b927e7\">live here.\u003c/a>\u003c/em>\u003c/p>\n\u003cp>Keep reading for everything you need to know about this uniquely Bay Area face-off.\u003c/p>\n\u003ch2>The taquería that started a soccer team\u003c/h2>\n\u003cp>If the San Francisco team name sounds familiar to you, that’s because, yes, it’s named after the longstanding local taquería chain El Farolito, with 12 locations all over the Bay Area.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>[pullquote size=\"medium\" align=\"right\" citation=\"Santiago López, head coach and general manager, El Farolito soccer team\"]‘The group is very motivated for this opportunity.’[/pullquote]The taquería chain’s founder Salvador López, who passed away in 2021, started the team in 1985, and whose players sport a bright yellow and blue soccer kit in the same color palette you’ll see in any of the El Farolito taquerías. Since its inception in 1985, the team — which has now risen to play in the semi-professional National Premier Soccer League (NPSL) — has charted a very successful path for itself, winning multiple regional and national championships.\u003c/p>\n\u003cp>El Farolito players balance all the responsibilities of being on the team with other full-time jobs. Some, like goalkeeper Julian Escobar, grew up in the Bay Area and came up playing for other local teams. But many in the team were recruited from professional teams across Latin America — striker Dembor Benson, for example, was a professional player in Honduras before joining El Farolito, \u003ca href=\"https://thecup.us/2024/04/15/2024-us-open-cup-round-2-dembor-benson-of-el-farolito-voted-thecup-us-player-of-the-round/\">where he has stood out in this year’s Open Cup, scoring the winning goal in the last two matches\u003c/a>.\u003c/p>\n\u003cp>And there’s a special energy this year among the team, says head coach and general manager Santiago López, who is Salvador’s son.\u003c/p>\n\u003cp>[aside postID=\"news_11961286,news_11952128,news_11915080\" label=\"Related Stories\"]The team started training in early January, much earlier than in previous years – something that combined with extra preseason games “really helped us out to get the team together and get into the competition mentality and the weekly routine,” López says. “If it wasn’t for the early start, we wouldn’t be in this type of rhythm.”\u003c/p>\n\u003ch2>‘Win it all or lose it all in one game’\u003c/h2>\n\u003cp>The El Farolito team has started the season without missing a single beat. The team is \u003ca href=\"https://www.npsl.com/schedule-2024/\">currently leading the standings for their conference in the National Premier Soccer League (NPSL\u003c/a>) with three wins and one draw. All of this is happening as they \u003ci>also \u003c/i>play in the Open Cup, where teams from all over the country compete in a knockout format.\u003c/p>\n\u003cp>It was El Farolito’s first win in this year’s competition — against Timbers 2, the reserve squad for the Portland Timbers of the Major League Soccer — \u003ca href=\"https://missionlocal.org/2024/03/burritooooooooooal-el-farolito-team-beats-major-league-soccer-affiliate/\">that brought renewed attention to the team and its unique standing in San Francisco’s Mission District\u003c/a>.\u003c/p>\n\u003cp>“We’ve done a lot more interviews and seen more photographers coming out,” López says of the heightened attention on his team. But his players nonetheless “still have a lot of ground to cover,” he says. “The group is very motivated for this opportunity.”\u003c/p>\n\u003cp>Motivation will be critical in Tuesday’s game against the Oakland Roots — the same team that knocked out El Farolito 3-1 in last year’s Open Cup.\u003c/p>\n\u003cp>The Roots, along with 15 other USL Championship clubs, \u003ca href=\"https://www.uslchampionship.com/news_article/show/1306095\">are joining the Open Cup in the third round due to competition rules\u003c/a>. The East Bay team is coming in hot after a 3-2 win against El Paso Locomotive in the USL Championship season, putting them back in the clear for playoffs. With two goals in that match, forward Johnny Rodriguez became the team’s all-time league scorer.\u003c/p>\n\u003cp>The knockout format of the Open Cup will make Tuesday’s game especially exciting, says Tommy Hodul, vice president of public relations for the Roots.\u003c/p>\n\u003cp>“You can win it all or lose it all in one game,” Hodul says, adding that “you have to prepare just as well as you do for a USL Championship game — no matter who the opponent is.”\u003c/p>\n\u003cp>Despite playing in different leagues, the Roots and El Farolito usually play each other during the preseason, and Hodul says his team is “well aware of what [El Farolito] brings, and the talent that they have on the roster.”\u003c/p>\n\u003cp>Playing against El Farolito, he says, is “a really good test for our guys getting ready for the USL Championship season.”\u003c/p>\n\u003ch2>Soccer is here to stay in the Bay\u003c/h2>\n\u003cp>For longtime soccer fans all over the Bay Area, Tuesday’s game is another example of how much soccer has grown in strength locally. In a time \u003ca href=\"https://www.kqed.org/news/11981876/oakland-as-relocate-to-sacramento-river-cats-home-stadium-for-3-seasons\">when other sports are seeing teams leave the Bay\u003c/a>, soccer’s role in the region’s identity has only grown.\u003c/p>\n\u003cp>Last month, the Bay FC kicked off their season — a first for the team and \u003ca href=\"https://www.kqed.org/news/11980330/a-new-pro-womens-soccer-team-kicks-off-in-the-bay\">for Northern California, its first National Women’s Soccer League team\u003c/a>. A year before that, Oakland Soul — part of the Roots organization — \u003ca href=\"https://www.kqed.org/news/11915080/oakland-roots-soccer-club-to-start-new-amateur-womens-team\">joined the USL W League\u003c/a>. And even the most casual of soccer fans had to admire the latest kit released by USL League Two’s San Francisco City FC, \u003ca href=\"https://twitter.com/SFCityFC/status/1772658868058730637/\">which features bright orange California poppies, Sutro Tower, the Golden Gate Bridge and the parrots that flock on Telegraph Hill\u003c/a>.\u003c/p>\n\u003cp>If El Farolito goes on to win the Open Cup, it would be a replay almost three decades in the making. The team already tasted championship glory in this competition back in 1993, when it went by the name of CD Mexico.\u003c/p>\n\u003cp>[ad floatright]\u003c/p>\n\u003cp>“We’re very focused on what we need to do,” coach López says.\u003c/p>\n\n","blocks":[],"excerpt":"After two wins, El Farolito faces off against the Oakland Roots on Tuesday in the third round of the U.S. Open Cup. Get the details on when and where to watch or stream the game.","status":"publish","parent":0,"modified":1713297553,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":25,"wordCount":1105},"headData":{"title":"A New Bay Area Clásico? SF's El Farolito and Oakland Roots Set to Battle in Hayward | KQED","description":"After two wins, El Farolito faces off against the Oakland Roots on Tuesday in the third round of the U.S. Open Cup. Get the details on when and where to watch or stream the game.","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/news/11983120/a-new-bay-area-clasico-sfs-el-farolito-and-oakland-roots-set-to-battle-in-hayward","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>Two Bay Area teams — one hailing from San Francisco and the other representing Oakland — face off on Tuesday.\u003c/p>\n\u003cp>Both teams boast storied histories and steadfast fans. But this isn’t the Giants and A’s we’re talking about, but rather \u003ca href=\"https://www.ussoccer.com/us-open-cup/watch?matchId=cd399be4-9cc2-4806-aeb9-dd2ae5b927e7\">San Francisco’s El Farolito soccer team vs. Oakland Roots Soccer Club\u003c/a>.\u003c/p>\n\u003cp>This crucial match, kicking off at Cal State East Bay’s Pioneer Stadium in Hayward at 7:30 p.m. on Tuesday, marks the third round of the \u003ca href=\"https://www.ussoccer.com/us-open-cup/\">U.S. Open Cup\u003c/a> — the oldest soccer competition in the country that brings teams together that usually play in different leagues.\u003c/p>\n\u003cp>\u003cem>Stream the game \u003ca href=\"https://www.ussoccer.com/us-open-cup/watch?matchId=cd399be4-9cc2-4806-aeb9-dd2ae5b927e7\">live here.\u003c/a>\u003c/em>\u003c/p>\n\u003cp>Keep reading for everything you need to know about this uniquely Bay Area face-off.\u003c/p>\n\u003ch2>The taquería that started a soccer team\u003c/h2>\n\u003cp>If the San Francisco team name sounds familiar to you, that’s because, yes, it’s named after the longstanding local taquería chain El Farolito, with 12 locations all over the Bay Area.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘The group is very motivated for this opportunity.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Santiago López, head coach and general manager, El Farolito soccer team","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>The taquería chain’s founder Salvador López, who passed away in 2021, started the team in 1985, and whose players sport a bright yellow and blue soccer kit in the same color palette you’ll see in any of the El Farolito taquerías. Since its inception in 1985, the team — which has now risen to play in the semi-professional National Premier Soccer League (NPSL) — has charted a very successful path for itself, winning multiple regional and national championships.\u003c/p>\n\u003cp>El Farolito players balance all the responsibilities of being on the team with other full-time jobs. Some, like goalkeeper Julian Escobar, grew up in the Bay Area and came up playing for other local teams. But many in the team were recruited from professional teams across Latin America — striker Dembor Benson, for example, was a professional player in Honduras before joining El Farolito, \u003ca href=\"https://thecup.us/2024/04/15/2024-us-open-cup-round-2-dembor-benson-of-el-farolito-voted-thecup-us-player-of-the-round/\">where he has stood out in this year’s Open Cup, scoring the winning goal in the last two matches\u003c/a>.\u003c/p>\n\u003cp>And there’s a special energy this year among the team, says head coach and general manager Santiago López, who is Salvador’s son.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11961286,news_11952128,news_11915080","label":"Related Stories "},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>The team started training in early January, much earlier than in previous years – something that combined with extra preseason games “really helped us out to get the team together and get into the competition mentality and the weekly routine,” López says. “If it wasn’t for the early start, we wouldn’t be in this type of rhythm.”\u003c/p>\n\u003ch2>‘Win it all or lose it all in one game’\u003c/h2>\n\u003cp>The El Farolito team has started the season without missing a single beat. The team is \u003ca href=\"https://www.npsl.com/schedule-2024/\">currently leading the standings for their conference in the National Premier Soccer League (NPSL\u003c/a>) with three wins and one draw. All of this is happening as they \u003ci>also \u003c/i>play in the Open Cup, where teams from all over the country compete in a knockout format.\u003c/p>\n\u003cp>It was El Farolito’s first win in this year’s competition — against Timbers 2, the reserve squad for the Portland Timbers of the Major League Soccer — \u003ca href=\"https://missionlocal.org/2024/03/burritooooooooooal-el-farolito-team-beats-major-league-soccer-affiliate/\">that brought renewed attention to the team and its unique standing in San Francisco’s Mission District\u003c/a>.\u003c/p>\n\u003cp>“We’ve done a lot more interviews and seen more photographers coming out,” López says of the heightened attention on his team. But his players nonetheless “still have a lot of ground to cover,” he says. “The group is very motivated for this opportunity.”\u003c/p>\n\u003cp>Motivation will be critical in Tuesday’s game against the Oakland Roots — the same team that knocked out El Farolito 3-1 in last year’s Open Cup.\u003c/p>\n\u003cp>The Roots, along with 15 other USL Championship clubs, \u003ca href=\"https://www.uslchampionship.com/news_article/show/1306095\">are joining the Open Cup in the third round due to competition rules\u003c/a>. The East Bay team is coming in hot after a 3-2 win against El Paso Locomotive in the USL Championship season, putting them back in the clear for playoffs. With two goals in that match, forward Johnny Rodriguez became the team’s all-time league scorer.\u003c/p>\n\u003cp>The knockout format of the Open Cup will make Tuesday’s game especially exciting, says Tommy Hodul, vice president of public relations for the Roots.\u003c/p>\n\u003cp>“You can win it all or lose it all in one game,” Hodul says, adding that “you have to prepare just as well as you do for a USL Championship game — no matter who the opponent is.”\u003c/p>\n\u003cp>Despite playing in different leagues, the Roots and El Farolito usually play each other during the preseason, and Hodul says his team is “well aware of what [El Farolito] brings, and the talent that they have on the roster.”\u003c/p>\n\u003cp>Playing against El Farolito, he says, is “a really good test for our guys getting ready for the USL Championship season.”\u003c/p>\n\u003ch2>Soccer is here to stay in the Bay\u003c/h2>\n\u003cp>For longtime soccer fans all over the Bay Area, Tuesday’s game is another example of how much soccer has grown in strength locally. In a time \u003ca href=\"https://www.kqed.org/news/11981876/oakland-as-relocate-to-sacramento-river-cats-home-stadium-for-3-seasons\">when other sports are seeing teams leave the Bay\u003c/a>, soccer’s role in the region’s identity has only grown.\u003c/p>\n\u003cp>Last month, the Bay FC kicked off their season — a first for the team and \u003ca href=\"https://www.kqed.org/news/11980330/a-new-pro-womens-soccer-team-kicks-off-in-the-bay\">for Northern California, its first National Women’s Soccer League team\u003c/a>. A year before that, Oakland Soul — part of the Roots organization — \u003ca href=\"https://www.kqed.org/news/11915080/oakland-roots-soccer-club-to-start-new-amateur-womens-team\">joined the USL W League\u003c/a>. And even the most casual of soccer fans had to admire the latest kit released by USL League Two’s San Francisco City FC, \u003ca href=\"https://twitter.com/SFCityFC/status/1772658868058730637/\">which features bright orange California poppies, Sutro Tower, the Golden Gate Bridge and the parrots that flock on Telegraph Hill\u003c/a>.\u003c/p>\n\u003cp>If El Farolito goes on to win the Open Cup, it would be a replay almost three decades in the making. The team already tasted championship glory in this competition back in 1993, when it went by the name of CD Mexico.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"floatright"},"numeric":["floatright"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>“We’re very focused on what we need to do,” coach López says.\u003c/p>\n\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983120/a-new-bay-area-clasico-sfs-el-farolito-and-oakland-roots-set-to-battle-in-hayward","authors":["11708"],"categories":["news_8","news_10"],"tags":["news_32793","news_27626","news_18","news_38","news_111","news_26124","news_28623"],"featImg":"news_11983111","label":"news"},"news_11983217":{"type":"posts","id":"news_11983217","meta":{"index":"posts_1591205157","site":"news","id":"11983217","found":true},"guestAuthors":[],"slug":"why-nearly-50-california-hospitals-were-forced-to-end-maternity-ward-services","title":"Why Nearly 50 California Hospitals Were Forced to End Maternity Ward Services","publishDate":1713380414,"format":"standard","headTitle":"Why Nearly 50 California Hospitals Were Forced to End Maternity Ward Services | KQED","labelTerm":{"term":18481,"site":"news"},"content":"\u003cp>In just the first few months of 2024, four California hospitals have closed or announced plans to close their maternity wards.\u003c/p>\n\u003cp>The closures are part of an accelerating trend unfolding across the state, creating maternity care deserts and decreasing access to prenatal care. In the past three years, 29 hospitals stopped delivering babies, according to a \u003ca href=\"https://calmatters.org/health/2023/11/california-hospitals-close-maternity-wards/\">CalMatters investigation on maternity ward closures\u003c/a>. Nearly 50 obstetrics departments have closed over the past decade.\u003c/p>\n\u003cp>Now, California lawmakers are trying to slow the trend.\u003c/p>\n\u003cp>Assemblymember \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/akilah-weber-165432\">Akilah Weber\u003c/a> and Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/dave-cortese-164699\">Dave Cortese\u003c/a> are pursuing legislation to increase transparency around planned maternity ward closures, potentially giving counties and the state time to intervene.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>Weber, a Democrat from La Mesa, wants hospitals to notify the state a year in advance if labor and delivery services are at risk of ending. The measure would also require the state to conduct a community impact report when a hospital indicates that it may lose maternity care.\u003c/p>\n\u003cp>Cortese, a Democrat from Campbell, wants to increase the public notification requirement of an impending closure from 90 days to 120 days and require the hospital to analyze how a closure could increase costs for the county health system, where the next-closest maternity wards are located and who is most likely to be affected.\u003c/p>\n\u003cp>Cortese’s bill would also require increased notification for planned closures of inpatient psychiatric services.\u003c/p>\n\u003cp>“We cannot continue to just discuss these issues and not implement policies to prevent or mitigate the harms and the continued disparities,” Weber said during an Assembly Health Committee hearing on Tuesday.\u003c/p>\n\u003cp>Groups representing doctors and reproductive health advocates support the measure. Nurses and consumer health advocates support Cortese’s bill.\u003c/p>\n\u003ch2>Why are California maternity wards closing?\u003c/h2>\n\u003cp>Ryan Spencer, a lobbyist for the regional chapter of the American College of Obstetricians and Gynecologists who testified in support of Weber’s measure, said there are often situations during birth where “every minute can be the difference between life and death.”\u003c/p>\n\u003cp>“What if you are a patient like this and literally had nowhere to go, who had to drive hours upon hours to get care? We have to find a way to end this crisis,” Spencer said during his testimony.[aside postID=news_11968835 hero='https://ww2.kqed.org/app/uploads/sites/10/2023/12/20231108-Alameda-Black-Maternal-Health-021-JY-qut-1020x680.jpg']Maternity wards are closing for several reasons, according to hospital administrators. They cite labor shortages, increasing costs, low reimbursements and declining birth rates.\u003c/p>\n\u003cp>The California Hospital Association opposes Cortese’s bill and has registered “concerns” about Weber’s. The group argues that neither bill will address the underlying reasons for maternity ward closures and may cause hospitals to terminate services sooner as employees leave and patients look elsewhere for care, said Kirsten Barlow, vice president of policy with the hospital association, during a Senate hearing earlier this month.\u003c/p>\n\u003cp>Current law requires hospitals to notify the public 90 days before a proposed service cut but doesn’t require the state to receive additional notification. Weber said that 90 days is “clearly not sufficient for the state to be able to intervene.”\u003c/p>\n\u003ch2>Maternity care deserts emerge\u003c/h2>\n\u003cp>CalMatters found that 12 counties have no hospital delivering babies, including Madera County, where the sudden closure of the county’s only hospital in 2022 spurred a flurry of emergency legislation supporting \u003ca href=\"https://calmatters.org/health/2023/08/california-hospitals-bailout-loans/\">distressed hospitals\u003c/a>.\u003c/p>\n\u003cp>\u003ca href=\"https://calmatters.org/health/2024/02/madera-hospital-reopen/\">Madera Community Hospital\u003c/a> is now on track to reopen but without a maternity ward. The company reopening the hospital, American Advanced Management, has indicated that low insurance reimbursement rates factored into its decision to open without labor and delivery.[aside postID=news_11976372 hero='https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/010423-MaderaCommunityHospital-LV_CM_07-copy-1020x680.jpg']“Reopening maternity would be like reopening two hospitals at the same time,” Matthew Beehler, chief strategy officer at American Advanced Management, previously told CalMatters.\u003c/p>\n\u003cp>Still, the bill authors and advocates are adamant that access to maternity care is a necessity. National studies indicate that \u003ca href=\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5885848/\">rates of preterm birth increase,\u003c/a> and \u003ca href=\"https://corey-white.com/assets/docs/frw_reduced_form_manuscript_AEJ_R1.pdf\">women receive less prenatal care\u003c/a> when labor and delivery units shut down, particularly in rural areas. CalMatters found that maternity closures in California disproportionately impact low-income and Latino communities.\u003c/p>\n\u003cp>“This is really a very simple bill. It doesn’t do much. It creates a public hearing opportunity at the local level to deal with issues that are …absolutely vital to the survival of our constituents,” Cortese said during a Senate Health Committee hearing on his measure.\u003c/p>\n\u003cp>\u003c/p>\n","blocks":[],"excerpt":"Two California lawmakers introduced bills intended to slow maternity ward closures after an investigation found nearly 50 hospitals had ended labor and delivery services between 2012 and 2023.","status":"publish","parent":0,"modified":1713380834,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":19,"wordCount":778},"headData":{"title":"Why Nearly 50 California Hospitals Were Forced to End Maternity Ward Services | KQED","description":"Two California lawmakers introduced bills intended to slow maternity ward closures after an investigation found nearly 50 hospitals had ended labor and delivery services between 2012 and 2023.","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"sticky":false,"nprByline":"Kristen Hwang, CalMatters","excludeFromSiteSearch":"Include","showOnAuthorArchivePages":"No","articleAge":"0","path":"/news/11983217/why-nearly-50-california-hospitals-were-forced-to-end-maternity-ward-services","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>In just the first few months of 2024, four California hospitals have closed or announced plans to close their maternity wards.\u003c/p>\n\u003cp>The closures are part of an accelerating trend unfolding across the state, creating maternity care deserts and decreasing access to prenatal care. In the past three years, 29 hospitals stopped delivering babies, according to a \u003ca href=\"https://calmatters.org/health/2023/11/california-hospitals-close-maternity-wards/\">CalMatters investigation on maternity ward closures\u003c/a>. Nearly 50 obstetrics departments have closed over the past decade.\u003c/p>\n\u003cp>Now, California lawmakers are trying to slow the trend.\u003c/p>\n\u003cp>Assemblymember \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/akilah-weber-165432\">Akilah Weber\u003c/a> and Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/dave-cortese-164699\">Dave Cortese\u003c/a> are pursuing legislation to increase transparency around planned maternity ward closures, potentially giving counties and the state time to intervene.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>Weber, a Democrat from La Mesa, wants hospitals to notify the state a year in advance if labor and delivery services are at risk of ending. The measure would also require the state to conduct a community impact report when a hospital indicates that it may lose maternity care.\u003c/p>\n\u003cp>Cortese, a Democrat from Campbell, wants to increase the public notification requirement of an impending closure from 90 days to 120 days and require the hospital to analyze how a closure could increase costs for the county health system, where the next-closest maternity wards are located and who is most likely to be affected.\u003c/p>\n\u003cp>Cortese’s bill would also require increased notification for planned closures of inpatient psychiatric services.\u003c/p>\n\u003cp>“We cannot continue to just discuss these issues and not implement policies to prevent or mitigate the harms and the continued disparities,” Weber said during an Assembly Health Committee hearing on Tuesday.\u003c/p>\n\u003cp>Groups representing doctors and reproductive health advocates support the measure. Nurses and consumer health advocates support Cortese’s bill.\u003c/p>\n\u003ch2>Why are California maternity wards closing?\u003c/h2>\n\u003cp>Ryan Spencer, a lobbyist for the regional chapter of the American College of Obstetricians and Gynecologists who testified in support of Weber’s measure, said there are often situations during birth where “every minute can be the difference between life and death.”\u003c/p>\n\u003cp>“What if you are a patient like this and literally had nowhere to go, who had to drive hours upon hours to get care? We have to find a way to end this crisis,” Spencer said during his testimony.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11968835","hero":"https://ww2.kqed.org/app/uploads/sites/10/2023/12/20231108-Alameda-Black-Maternal-Health-021-JY-qut-1020x680.jpg","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>Maternity wards are closing for several reasons, according to hospital administrators. They cite labor shortages, increasing costs, low reimbursements and declining birth rates.\u003c/p>\n\u003cp>The California Hospital Association opposes Cortese’s bill and has registered “concerns” about Weber’s. The group argues that neither bill will address the underlying reasons for maternity ward closures and may cause hospitals to terminate services sooner as employees leave and patients look elsewhere for care, said Kirsten Barlow, vice president of policy with the hospital association, during a Senate hearing earlier this month.\u003c/p>\n\u003cp>Current law requires hospitals to notify the public 90 days before a proposed service cut but doesn’t require the state to receive additional notification. Weber said that 90 days is “clearly not sufficient for the state to be able to intervene.”\u003c/p>\n\u003ch2>Maternity care deserts emerge\u003c/h2>\n\u003cp>CalMatters found that 12 counties have no hospital delivering babies, including Madera County, where the sudden closure of the county’s only hospital in 2022 spurred a flurry of emergency legislation supporting \u003ca href=\"https://calmatters.org/health/2023/08/california-hospitals-bailout-loans/\">distressed hospitals\u003c/a>.\u003c/p>\n\u003cp>\u003ca href=\"https://calmatters.org/health/2024/02/madera-hospital-reopen/\">Madera Community Hospital\u003c/a> is now on track to reopen but without a maternity ward. The company reopening the hospital, American Advanced Management, has indicated that low insurance reimbursement rates factored into its decision to open without labor and delivery.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11976372","hero":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/02/010423-MaderaCommunityHospital-LV_CM_07-copy-1020x680.jpg","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>“Reopening maternity would be like reopening two hospitals at the same time,” Matthew Beehler, chief strategy officer at American Advanced Management, previously told CalMatters.\u003c/p>\n\u003cp>Still, the bill authors and advocates are adamant that access to maternity care is a necessity. National studies indicate that \u003ca href=\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5885848/\">rates of preterm birth increase,\u003c/a> and \u003ca href=\"https://corey-white.com/assets/docs/frw_reduced_form_manuscript_AEJ_R1.pdf\">women receive less prenatal care\u003c/a> when labor and delivery units shut down, particularly in rural areas. CalMatters found that maternity closures in California disproportionately impact low-income and Latino communities.\u003c/p>\n\u003cp>“This is really a very simple bill. It doesn’t do much. It creates a public hearing opportunity at the local level to deal with issues that are …absolutely vital to the survival of our constituents,” Cortese said during a Senate Health Committee hearing on his measure.\u003c/p>\n\u003cp>\u003c/p>\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983217/why-nearly-50-california-hospitals-were-forced-to-end-maternity-ward-services","authors":["byline_news_11983217"],"categories":["news_457","news_8"],"tags":["news_18538","news_18543","news_18659","news_33578","news_21771","news_33583"],"affiliates":["news_18481"],"featImg":"news_11983218","label":"news_18481"},"forum_2010101905416":{"type":"posts","id":"forum_2010101905416","meta":{"index":"posts_1591205157","site":"forum","id":"2010101905416","found":true},"guestAuthors":[],"slug":"what-the-99-cents-only-stores-closure-means-to-californians","title":"What the 99 Cents Only Stores Closure Means to Californians","publishDate":1713310947,"format":"audio","headTitle":"What the 99 Cents Only Stores Closure Means to Californians | KQED","labelTerm":{"site":"forum"},"content":"\u003cp>Dollar stores – the bargain chains prevalent in rural areas that sell miscellaneous merchandise at steeply discounted prices – have been blamed for contributing to food deserts and pushing out smaller mom and pop grocers. But the 99 Cents Only chain stood for something different to its fans, according to LA Times reporter Andrea Chang, who says that people relied on the bright and well-organized spaces for good quality merchandise. The California-based company announced that it will be closing all 371 of its stores just as another prominent chain, Family Dollar, plans to shutter 1000 stores. We’ll talk about the history of dollar stores, the impact they have on communities across the country and what happens to the people reliant on them when they leave.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\u003cp>\u003c/p>\n","blocks":[],"excerpt":"We’ll talk about the history of dollar stores, the impact they have on communities across the country and what happens to the people reliant on them when they leave.","status":"publish","parent":0,"modified":1713379964,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":3,"wordCount":131},"headData":{"title":"What the 99 Cents Only Stores Closure Means to Californians | KQED","description":"We’ll talk about the history of dollar stores, the impact they have on communities across the country and what happens to the people reliant on them when they leave.","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"audioUrl":"https://www.podtrac.com/pts/redirect.mp3/pdst.fm/e/chrt.fm/track/G6C7C3/traffic.megaphone.fm/KQINC5649387615.mp3?updated=1713379368","airdate":1713373200,"forumGuests":[{"name":"Eliza Ronalds-Hannon","bio":"senior reporter, Bloomberg"},{"name":"Andrea Chang","bio":"wealth reporter, Los Angeles Times"},{"name":"Sara Portnoy","bio":"professor of Latinx food studies and food justice, USC; creator and executive producer of \"Abuelitas on the Borderlands\" film series"}],"sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/forum/2010101905416/what-the-99-cents-only-stores-closure-means-to-californians","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>Dollar stores – the bargain chains prevalent in rural areas that sell miscellaneous merchandise at steeply discounted prices – have been blamed for contributing to food deserts and pushing out smaller mom and pop grocers. But the 99 Cents Only chain stood for something different to its fans, according to LA Times reporter Andrea Chang, who says that people relied on the bright and well-organized spaces for good quality merchandise. The California-based company announced that it will be closing all 371 of its stores just as another prominent chain, Family Dollar, plans to shutter 1000 stores. We’ll talk about the history of dollar stores, the impact they have on communities across the country and what happens to the people reliant on them when they leave.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\u003cp>\u003c/p>\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/forum/2010101905416/what-the-99-cents-only-stores-closure-means-to-californians","authors":["243"],"categories":["forum_165"],"featImg":"forum_2010101905423","label":"forum"},"news_11983180":{"type":"posts","id":"news_11983180","meta":{"index":"posts_1591205157","site":"news","id":"11983180","found":true},"guestAuthors":[],"slug":"democrats-kill-california-homeless-camp-ban-again","title":"Democrats Again Vote Down California Ban on Unhoused Encampments","publishDate":1713351657,"format":"standard","headTitle":"Democrats Again Vote Down California Ban on Unhoused Encampments | KQED","labelTerm":{"term":18481,"site":"news"},"content":"\u003cp>For the second year in a row, Democrats voted down a bill on Tuesday that sought to ban homeless encampments near schools, transit stops and other areas throughout California.\u003c/p>\n\u003cp>Even though cities up and down the state are grappling with a proliferation of homeless camps, legislators said they oppose penalizing down-and-out residents who sleep on public property.[aside postID=news_11983000 hero='https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-1020x705.jpg']“Just because individuals that are unhoused make people uncomfortable does not mean that it should be criminalized. And this bill does that,” said Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/aisha-wahab-165437\">Aisha Wahab\u003c/a>, a Democrat from Fremont and chairperson of the Senate Public Safety Committee. “The penalties will just be added to their already difficult situation of paying for things.”\u003c/p>\n\u003cp>\u003ca href=\"https://digitaldemocracy.calmatters.org/bills/ca_202320240sb1011?slug=CA_202320240SB1011&_gl=1*12wezuh*_ga*Nzc5MjE5NDU2LjE2ODQ1MTA1NDg.*_ga_5TKXNLE5NK*MTcxMzI5MTE2MC4zNTAuMS4xNzEzMjk2OTk3LjYwLjAuMA..*_ga_GNY4L81DZE*MTcxMzI5MTE2MC4yOTYuMS4xNzEzMjk1NjgwLjAuMC4w\">Senate Bill 1011\u003c/a> stumbled in its first committee hearing, stalling in the Public Safety Committee on a 1–3 vote. The measure by Senate GOP leader \u003ca href=\"https://calmatters.org/legislator-tracker/brian-jones-1968/?utm_source=CalMatters%20Newsletters&utm_campaign=5df65efca8-WHATMATTERS&utm_medium=email&utm_term=0_faa7be558d-5df65efca8-151973523&mc_cid=5df65efca8&mc_eid=df84c5373c\">Brian Jones\u003c/a> and Democratic Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/catherine-blakespear-21275\">Catherine Blakespear\u003c/a>, both of the San Diego area, would have made camping within 500 feet of a school, open space or major transit stop a misdemeanor or infraction. It also would have banned camping on public sidewalks if beds were available in local homeless shelters.\u003c/p>\n\u003cp>“I’m disappointed in the closed-minded opposition from the majority party members of the Senate Public Safety Committee to new approaches and their knee-jerk support of just throwing more money at the problem with no real plan,” Jones said in a statement. “Today’s continued rejection of real solutions during this health and safety crisis is immoral and irresponsible.”\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>After today’s defeat, Jones will continue speaking with committee members to see if there is any way to negotiate a path forward for his bill, spokesperson Nina Krishel said in an email.\u003c/p>\n\u003cp>Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/nancy-skinner-34364\">Nancy Skinner\u003c/a>, a Democrat from Oakland, said while she appreciates that Californians don’t want to see encampments, she couldn’t support the bill.\u003c/p>\n\u003cp>“It’s kind of like trying to make a problem invisible versus addressing the core of the problem,” said Skinner, who joined Wahab and Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/scott-wiener-100936\">Scott Wiener\u003c/a>, a Democrat from San Francisco, in voting “no.”\u003c/p>\n\u003cp>More than three dozen people voiced their opposition to the bill during today’s hearing, speaking on behalf of organizations such as the Ella Baker Center for Human Rights and the American Civil Liberties Union California Action.[aside postID=news_11982817 hero='https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240410-HMB-Farmworkers-TH-01-KQED-1020x680.jpg']The bill’s supporters, who numbered far fewer, included the mayor of Vista and a representative from the city of Carlsbad.\u003c/p>\n\u003cp>The lone “yes” vote came from the committee’s only Republican, Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/kelly-seyarto-165446\">Kelly Seyarto\u003c/a> of Murrieta.\u003c/p>\n\u003cp>“We had a slew of people that came forward to tell us about what we shouldn’t be doing,” he said. “But what the hell should we be doing? Because right now, we’re not doing anything.”\u003c/p>\n\u003cp>Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/steven-bradford-100945\">Steven Bradford\u003c/a>, a Democrat from Inglewood, abstained.\u003c/p>\n\u003cp>Wahab granted reconsideration, which means the committee could hear the bill again later this session. But last year, a nearly identical bill \u003ca href=\"https://calmatters.org/newsletters/whatmatters/2023/03/california-homeless-encampments/\">met the same fate\u003c/a>. SB 31, also introduced by Jones, died in the Senate Public Safety Committee with one “yes” vote, one “no” vote and three abstentions. It also received reconsideration but was never revived.\u003c/p>\n\u003cp>This year’s version of the encampment ban had more going for it. Jones found a Democratic co-author and narrowed the bill’s scope. Instead of banning people from camping within 1,000 feet of schools and other locations, the new bill would have banned people from camping within 500 feet.\u003c/p>\n\u003cp>Jones also was leaning heavily on a new camping ban in San Diego, upon which he said he modeled his bill. The San Diego ordinance, which took effect at the end of July 2023, bans camps near schools, shelters and transit hubs, in parks, and — if shelter beds are available — on public sidewalks. Jones called the ordinance a “success,” a sentiment echoed by San Diego Mayor Todd Gloria.\u003c/p>\n\u003cp>But a \u003ca href=\"https://calmatters.org/housing/homelessness/2024/04/homeless-encampment-ban/\">CalMatters investigation\u003c/a> paints a more complicated picture. While encampments have drastically decreased in some areas, such as downtown and around certain schools, they are still just as prevalent — in some cases much more so — along the city’s freeways and the banks of its river. Opponents of the ordinance say it displaces people instead of housing them.\u003c/p>\n\u003cp>And Jones’ bill failed to copy a key piece of San Diego’s approach. When the city started enforcing its encampment ban, it also opened two massive “safe sleeping” sites where about 500 people camp on vacant lots in tents purchased by the city.\u003c/p>\n\u003cp>Jones’ bill would not have forced cities to set up accommodations for people displaced from encampments because, he said, there’s no state funding for that.\u003c/p>\n\u003cp>\u003c/p>\n","blocks":[],"excerpt":"A bill to ban unhoused encampments statewide near parks, schools and transit hubs failed to get out of the same legislative committee as last year.","status":"publish","parent":0,"modified":1713314219,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":19,"wordCount":871},"headData":{"title":"Democrats Again Vote Down California Ban on Unhoused Encampments | KQED","description":"A bill to ban unhoused encampments statewide near parks, schools and transit hubs failed to get out of the same legislative committee as last year.","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"sticky":false,"nprByline":"Marisa Kendall, CalMatters","excludeFromSiteSearch":"Include","showOnAuthorArchivePages":"No","articleAge":"0","path":"/news/11983180/democrats-kill-california-homeless-camp-ban-again","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>For the second year in a row, Democrats voted down a bill on Tuesday that sought to ban homeless encampments near schools, transit stops and other areas throughout California.\u003c/p>\n\u003cp>Even though cities up and down the state are grappling with a proliferation of homeless camps, legislators said they oppose penalizing down-and-out residents who sleep on public property.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11983000","hero":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/GettyImages-623874284_qut-1020x705.jpg","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>“Just because individuals that are unhoused make people uncomfortable does not mean that it should be criminalized. And this bill does that,” said Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/aisha-wahab-165437\">Aisha Wahab\u003c/a>, a Democrat from Fremont and chairperson of the Senate Public Safety Committee. “The penalties will just be added to their already difficult situation of paying for things.”\u003c/p>\n\u003cp>\u003ca href=\"https://digitaldemocracy.calmatters.org/bills/ca_202320240sb1011?slug=CA_202320240SB1011&_gl=1*12wezuh*_ga*Nzc5MjE5NDU2LjE2ODQ1MTA1NDg.*_ga_5TKXNLE5NK*MTcxMzI5MTE2MC4zNTAuMS4xNzEzMjk2OTk3LjYwLjAuMA..*_ga_GNY4L81DZE*MTcxMzI5MTE2MC4yOTYuMS4xNzEzMjk1NjgwLjAuMC4w\">Senate Bill 1011\u003c/a> stumbled in its first committee hearing, stalling in the Public Safety Committee on a 1–3 vote. The measure by Senate GOP leader \u003ca href=\"https://calmatters.org/legislator-tracker/brian-jones-1968/?utm_source=CalMatters%20Newsletters&utm_campaign=5df65efca8-WHATMATTERS&utm_medium=email&utm_term=0_faa7be558d-5df65efca8-151973523&mc_cid=5df65efca8&mc_eid=df84c5373c\">Brian Jones\u003c/a> and Democratic Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/catherine-blakespear-21275\">Catherine Blakespear\u003c/a>, both of the San Diego area, would have made camping within 500 feet of a school, open space or major transit stop a misdemeanor or infraction. It also would have banned camping on public sidewalks if beds were available in local homeless shelters.\u003c/p>\n\u003cp>“I’m disappointed in the closed-minded opposition from the majority party members of the Senate Public Safety Committee to new approaches and their knee-jerk support of just throwing more money at the problem with no real plan,” Jones said in a statement. “Today’s continued rejection of real solutions during this health and safety crisis is immoral and irresponsible.”\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>After today’s defeat, Jones will continue speaking with committee members to see if there is any way to negotiate a path forward for his bill, spokesperson Nina Krishel said in an email.\u003c/p>\n\u003cp>Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/nancy-skinner-34364\">Nancy Skinner\u003c/a>, a Democrat from Oakland, said while she appreciates that Californians don’t want to see encampments, she couldn’t support the bill.\u003c/p>\n\u003cp>“It’s kind of like trying to make a problem invisible versus addressing the core of the problem,” said Skinner, who joined Wahab and Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/scott-wiener-100936\">Scott Wiener\u003c/a>, a Democrat from San Francisco, in voting “no.”\u003c/p>\n\u003cp>More than three dozen people voiced their opposition to the bill during today’s hearing, speaking on behalf of organizations such as the Ella Baker Center for Human Rights and the American Civil Liberties Union California Action.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11982817","hero":"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/240410-HMB-Farmworkers-TH-01-KQED-1020x680.jpg","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>The bill’s supporters, who numbered far fewer, included the mayor of Vista and a representative from the city of Carlsbad.\u003c/p>\n\u003cp>The lone “yes” vote came from the committee’s only Republican, Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/kelly-seyarto-165446\">Kelly Seyarto\u003c/a> of Murrieta.\u003c/p>\n\u003cp>“We had a slew of people that came forward to tell us about what we shouldn’t be doing,” he said. “But what the hell should we be doing? Because right now, we’re not doing anything.”\u003c/p>\n\u003cp>Sen. \u003ca href=\"https://digitaldemocracy.calmatters.org/legislators/steven-bradford-100945\">Steven Bradford\u003c/a>, a Democrat from Inglewood, abstained.\u003c/p>\n\u003cp>Wahab granted reconsideration, which means the committee could hear the bill again later this session. But last year, a nearly identical bill \u003ca href=\"https://calmatters.org/newsletters/whatmatters/2023/03/california-homeless-encampments/\">met the same fate\u003c/a>. SB 31, also introduced by Jones, died in the Senate Public Safety Committee with one “yes” vote, one “no” vote and three abstentions. It also received reconsideration but was never revived.\u003c/p>\n\u003cp>This year’s version of the encampment ban had more going for it. Jones found a Democratic co-author and narrowed the bill’s scope. Instead of banning people from camping within 1,000 feet of schools and other locations, the new bill would have banned people from camping within 500 feet.\u003c/p>\n\u003cp>Jones also was leaning heavily on a new camping ban in San Diego, upon which he said he modeled his bill. The San Diego ordinance, which took effect at the end of July 2023, bans camps near schools, shelters and transit hubs, in parks, and — if shelter beds are available — on public sidewalks. Jones called the ordinance a “success,” a sentiment echoed by San Diego Mayor Todd Gloria.\u003c/p>\n\u003cp>But a \u003ca href=\"https://calmatters.org/housing/homelessness/2024/04/homeless-encampment-ban/\">CalMatters investigation\u003c/a> paints a more complicated picture. While encampments have drastically decreased in some areas, such as downtown and around certain schools, they are still just as prevalent — in some cases much more so — along the city’s freeways and the banks of its river. Opponents of the ordinance say it displaces people instead of housing them.\u003c/p>\n\u003cp>And Jones’ bill failed to copy a key piece of San Diego’s approach. When the city started enforcing its encampment ban, it also opened two massive “safe sleeping” sites where about 500 people camp on vacant lots in tents purchased by the city.\u003c/p>\n\u003cp>Jones’ bill would not have forced cities to set up accommodations for people displaced from encampments because, he said, there’s no state funding for that.\u003c/p>\n\u003cp>\u003c/p>\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983180/democrats-kill-california-homeless-camp-ban-again","authors":["byline_news_11983180"],"categories":["news_6266","news_8"],"tags":["news_18538","news_22307","news_33966","news_27626","news_21214","news_4020","news_1775"],"affiliates":["news_18481"],"featImg":"news_11983184","label":"news_18481"},"news_11983000":{"type":"posts","id":"news_11983000","meta":{"index":"posts_1591205157","site":"news","id":"11983000","found":true},"guestAuthors":[],"slug":"california-legislators-take-aim-at-construction-fees-to-boost-housing","title":"California Legislators Take Aim at Construction Fees to Boost Housing","publishDate":1713277810,"format":"standard","headTitle":"California Legislators Take Aim at Construction Fees to Boost Housing | KQED","labelTerm":{"site":"news"},"content":"\u003cp>After nearly a decade of trying to peel away the red tape holding back housing construction in California, legislators this year are nibbling away at the last of the low-hanging fruit: impact fees.\u003c/p>\n\u003cp>Cities impose impact fees to fund construction for new schools, road maintenance, public art installations, and other amenities. The fees vary widely based on the type of project and city — ranging from \u003ca href=\"https://ternercenter.berkeley.edu/development-fees\">as low as $12,000 per unit to as high as $157,000 per unit\u003c/a>.[pullquote size=\"medium\" align=\"right\" citation=\"Erik Schoennauer, land use consultant\"]‘The city should create a master list of all potential fees, anything conceivable.’[/pullquote]\u003c/p>\n\u003cp>“These can be really, really high costs that can make or break the math on a development,” said Sean Roberts, a developer and CEO of Villa Homes. “These fees create a barrier to actually getting homes built, and that’s not good for anybody right now in California.”\u003c/p>\n\u003cp>The constitutionality of these fees was recently challenged in the Supreme Court. Last week, the court unanimously ruled that cities should have to demonstrate the fees they are charging are reasonable. But, they left it to lower courts to decide what counts as a reasonable fee. Meaning, there won’t be any immediate changes to how much cities are charging.\u003c/p>\n\u003cp>In the meantime, a slate of bills is making its way through the legislature. None of the bills would actually reduce these fees. That’s because doing so would require tackling a much thornier question of how to make up for cities’ lost revenue. Instead, these bills aim to address other issues that developers have with the fees: that they don’t often know going into a project how much the fees will cost and that they are often due before projects even break ground.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>[aside postID=\"news_11981595,news_11945744,news_11980019\" label=\"Related Stories\"]SB 937 would make payment due only once people are actually living in the new housing. AB 2144, authored by Assemblymember Timothy Grayson (D-Concord), and AB 1820, authored by Assemblymember Pilar Schiavo (D-Santa Clarita), would both require cities to post easily accessible information about the fees they charge. And a fifth bill, AB 1210, would cap the fees developers have to pay to connect new homes and apartment buildings to utility services, limiting the fees to 1% of the project’s estimated value.\u003c/p>\n\u003cp>As the cost of materials, labor and interest rates continue to soar, legislators see these changes as one of the last remaining levers they can pull to reduce the cost of construction and spur development across the state. And while developers generally welcome these efforts to make housing easier to build, they say there are much bigger, meatier fish to fry in the complicated politics of California housing construction.\u003c/p>\n\u003cp>Erik Schoennauer, a land use consultant who works with developers in San Jose, said he’s been advocating for the changes the bills propose for years. As it stands, he said, “there is no one-stop location” to understand what fees are due and when.\u003c/p>\n\u003cp>“The city should create a master list of all potential fees, anything conceivable,” Schoennauer said. “It’s much harder to determine what [fees] apply when you don’t even know what the maximum list is.”\u003c/p>\n\u003cp>AB 2144 would require cities to post information on impact fee schedules, along with a “nexus study,” which would break down the total cost of construction on a city’s website. AB 1820 mandates cities provide an estimate of the fees developers would have to pay within 10 days of a developer filing an application.\u003c/p>\n\u003cp>But the problems surrounding fees are much deeper than a lack of transparency, Roberts said. His company specializes in constructing prefabricated granny flats and in-law units homeowners can put in their backyards. For the past few months, he’s also been working on building clusters of small homes called cottage courts.\u003c/p>\n\u003cfigure id=\"attachment_11983026\" class=\"wp-caption aligncenter\" style=\"max-width: 1920px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11983026\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut.jpg\" alt=\"An aerial view of a green house with a solar panel on the roof and a yard.\" width=\"1920\" height=\"1440\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut.jpg 1920w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-800x600.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-1020x765.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-160x120.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-1536x1152.jpg 1536w\" sizes=\"(max-width: 1920px) 100vw, 1920px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">While Villa Homes specializes in constructing prefabricated granny flats and in-law units, the company has started to branch out into building small and affordable single-family homes. According to Roberts, impact fees raise costs and can make these homes unaffordable. \u003ccite>(Courtesy Villa Homes)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>By design, these homes are smaller and, therefore, meant to be more affordable to purchase than a standard single-family home. But as he’s put together budget sheets for these projects, the impact fees have started to add up.\u003c/p>\n\u003cp>“The impact fees that we often run into in many jurisdictions don’t scale down, even though we’re building a smaller home at a lower price point,” he said. “At the end of the day, we want to get people into homes they can afford to buy and to do that on a private market without a bunch of government subsidies.”\u003c/p>\n\u003cp>SB 937 would push impact fees to be due once the homes are sold, but Roberts said that would only be “moving money through time.”\u003c/p>\n\u003cp>“The cost is still there,” he said. “It’s just going to be borne later in the project and ultimately by the [occupant].”\u003c/p>\n\u003cp>Sen. Scott Wiener (D- San Francisco) said he authored this bill to help developers with the upfront costs of construction but acknowledged that there is a much larger conversation still to be had about how cities rationalize exorbitant fees that can kill projects while claiming to want more housing.\u003c/p>\n\u003cp>“There are cities where the impact fees are way too high,” he said. “They’re out of whack, and they’re harming the ability of housing to be built.”\u003c/p>\n\u003cp>The high cost of these fees was at the heart of the case that went to the Supreme Court. In 2016, contractor George Sheetz was preparing to build a small home on a vacant lot in El Dorado County, but the county charged $23,000 for a “traffic impact fee,” even though, Sheetz alleged, there was no evidence the development would lead to more traffic.\u003c/p>\n\u003cp>On Friday, the U.S. Supreme Court ruled unanimously in favor of Sheetz, saying developers have a right to challenge the constitutionality of these fees. Though the case’s fate ultimately rests in a lower court, the high court’s ruling could mean more developers will take cities to court over what Sheetz argued was “extortionate fees.”\u003c/p>\n\u003cp>“The way impact fees have thus far been imposed has been arbitrary and varies widely from town to town,” Jim Wunderman, President and CEO of the Bay Area Council said in a \u003ca href=\"https://www.bayareacouncil.org/press-releases/bay-area-council-hails-supreme-court-decision-on-costly-impact-fees/\">statement\u003c/a>. The regional business advocacy organization was one of many to submit amicus briefs in favor of Sheetz’s case. “This ruling is hopefully the first step on the path to returning some fairness in how housing and other local impact fees are charged.”\u003c/p>\n\u003cp>Many cities, however, rely on these fees to fund government services and city maintenance. Jason Rhine, director of legislative affairs for the League of California Cities, argues impact fees simply account for more people living in a city once the new housing is built.\u003c/p>\n\u003cp>“Most cities do not have a lot of excess dollars lying around in their general fund to help subsidize these [new] projects,” he said. “Developers have to pay their fair share when it comes to the impact that project is going to have on their community.”\u003c/p>\n\u003cp>When voters in 1978 passed Proposition 13, which limits the amount cities can increase property taxes each year, this revenue accounted for 90% of a city’s total income. According to a \u003ca href=\"https://lao.ca.gov/Publications/Report/3497#How_Did_Proposition.A013_Change_Local_Governments_Mix_of_Tax_Revenues.3F\">study from the Legislative Analyst’s Office\u003c/a>, that share in 2016 was less than two-thirds.\u003c/p>\n\u003cp>“The biggest reason why impact fees are so pricey is due to municipal governments not having many ways to levy taxes,” said Muhammad Alameldin, a policy associate at UC Berkeley’s Terner Center for Housing Innovation.\u003c/p>\n\u003cp>Because Proposition 13 has artificially suppressed property tax revenue for decades, cities can no longer rely on property owners to foot the bill for maintaining their neighborhoods. Cities with fewer commercial centers, like San Jose or other suburban municipalities, are, therefore, in a tighter bind to find revenue.\u003c/p>\n\u003cp>Wiener said he was sympathetic to cities’ plight.\u003c/p>\n\u003cp>“We made it really hard for them to fund basic municipal services,” he said. “So, that’s why they have become overly reliant on impact fees on new housing.”\u003c/p>\n\u003cp>And he acknowledged that he and other lawmakers are kicking the can down the road on a much larger — and more meaningful — conversation.\u003c/p>\n\u003cp>[ad floatright]\u003c/p>\n\u003cp>“The much broader issue is how cities are funded in California,” Wiener said. “[My] bill is not a substitute for the broader conversation.”\u003c/p>\n\n","blocks":[],"excerpt":"Cities rely on impact fees to maintain parks, schools and other amenities. But developers say the fees can prevent housing from being built. A series of new bills try to find a middle ground.","status":"publish","parent":0,"modified":1713292384,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":31,"wordCount":1505},"headData":{"title":"California Legislators Take Aim at Construction Fees to Boost Housing | KQED","description":"Cities rely on impact fees to maintain parks, schools and other amenities. But developers say the fees can prevent housing from being built. A series of new bills try to find a middle ground.","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/news/11983000/california-legislators-take-aim-at-construction-fees-to-boost-housing","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>After nearly a decade of trying to peel away the red tape holding back housing construction in California, legislators this year are nibbling away at the last of the low-hanging fruit: impact fees.\u003c/p>\n\u003cp>Cities impose impact fees to fund construction for new schools, road maintenance, public art installations, and other amenities. The fees vary widely based on the type of project and city — ranging from \u003ca href=\"https://ternercenter.berkeley.edu/development-fees\">as low as $12,000 per unit to as high as $157,000 per unit\u003c/a>.\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"‘The city should create a master list of all potential fees, anything conceivable.’","name":"pullquote","attributes":{"named":{"size":"medium","align":"right","citation":"Erik Schoennauer, land use consultant","label":""},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>“These can be really, really high costs that can make or break the math on a development,” said Sean Roberts, a developer and CEO of Villa Homes. “These fees create a barrier to actually getting homes built, and that’s not good for anybody right now in California.”\u003c/p>\n\u003cp>The constitutionality of these fees was recently challenged in the Supreme Court. Last week, the court unanimously ruled that cities should have to demonstrate the fees they are charging are reasonable. But, they left it to lower courts to decide what counts as a reasonable fee. Meaning, there won’t be any immediate changes to how much cities are charging.\u003c/p>\n\u003cp>In the meantime, a slate of bills is making its way through the legislature. None of the bills would actually reduce these fees. That’s because doing so would require tackling a much thornier question of how to make up for cities’ lost revenue. Instead, these bills aim to address other issues that developers have with the fees: that they don’t often know going into a project how much the fees will cost and that they are often due before projects even break ground.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11981595,news_11945744,news_11980019","label":"Related Stories "},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>SB 937 would make payment due only once people are actually living in the new housing. AB 2144, authored by Assemblymember Timothy Grayson (D-Concord), and AB 1820, authored by Assemblymember Pilar Schiavo (D-Santa Clarita), would both require cities to post easily accessible information about the fees they charge. And a fifth bill, AB 1210, would cap the fees developers have to pay to connect new homes and apartment buildings to utility services, limiting the fees to 1% of the project’s estimated value.\u003c/p>\n\u003cp>As the cost of materials, labor and interest rates continue to soar, legislators see these changes as one of the last remaining levers they can pull to reduce the cost of construction and spur development across the state. And while developers generally welcome these efforts to make housing easier to build, they say there are much bigger, meatier fish to fry in the complicated politics of California housing construction.\u003c/p>\n\u003cp>Erik Schoennauer, a land use consultant who works with developers in San Jose, said he’s been advocating for the changes the bills propose for years. As it stands, he said, “there is no one-stop location” to understand what fees are due and when.\u003c/p>\n\u003cp>“The city should create a master list of all potential fees, anything conceivable,” Schoennauer said. “It’s much harder to determine what [fees] apply when you don’t even know what the maximum list is.”\u003c/p>\n\u003cp>AB 2144 would require cities to post information on impact fee schedules, along with a “nexus study,” which would break down the total cost of construction on a city’s website. AB 1820 mandates cities provide an estimate of the fees developers would have to pay within 10 days of a developer filing an application.\u003c/p>\n\u003cp>But the problems surrounding fees are much deeper than a lack of transparency, Roberts said. His company specializes in constructing prefabricated granny flats and in-law units homeowners can put in their backyards. For the past few months, he’s also been working on building clusters of small homes called cottage courts.\u003c/p>\n\u003cfigure id=\"attachment_11983026\" class=\"wp-caption aligncenter\" style=\"max-width: 1920px\">\u003ca href=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut.jpg\">\u003cimg loading=\"lazy\" decoding=\"async\" class=\"size-full wp-image-11983026\" src=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut.jpg\" alt=\"An aerial view of a green house with a solar panel on the roof and a yard.\" width=\"1920\" height=\"1440\" srcset=\"https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut.jpg 1920w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-800x600.jpg 800w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-1020x765.jpg 1020w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-160x120.jpg 160w, https://cdn.kqed.org/wp-content/uploads/sites/10/2024/04/Overlook-151_qut-1536x1152.jpg 1536w\" sizes=\"(max-width: 1920px) 100vw, 1920px\">\u003c/a>\u003cfigcaption class=\"wp-caption-text\">While Villa Homes specializes in constructing prefabricated granny flats and in-law units, the company has started to branch out into building small and affordable single-family homes. According to Roberts, impact fees raise costs and can make these homes unaffordable. \u003ccite>(Courtesy Villa Homes)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>By design, these homes are smaller and, therefore, meant to be more affordable to purchase than a standard single-family home. But as he’s put together budget sheets for these projects, the impact fees have started to add up.\u003c/p>\n\u003cp>“The impact fees that we often run into in many jurisdictions don’t scale down, even though we’re building a smaller home at a lower price point,” he said. “At the end of the day, we want to get people into homes they can afford to buy and to do that on a private market without a bunch of government subsidies.”\u003c/p>\n\u003cp>SB 937 would push impact fees to be due once the homes are sold, but Roberts said that would only be “moving money through time.”\u003c/p>\n\u003cp>“The cost is still there,” he said. “It’s just going to be borne later in the project and ultimately by the [occupant].”\u003c/p>\n\u003cp>Sen. Scott Wiener (D- San Francisco) said he authored this bill to help developers with the upfront costs of construction but acknowledged that there is a much larger conversation still to be had about how cities rationalize exorbitant fees that can kill projects while claiming to want more housing.\u003c/p>\n\u003cp>“There are cities where the impact fees are way too high,” he said. “They’re out of whack, and they’re harming the ability of housing to be built.”\u003c/p>\n\u003cp>The high cost of these fees was at the heart of the case that went to the Supreme Court. In 2016, contractor George Sheetz was preparing to build a small home on a vacant lot in El Dorado County, but the county charged $23,000 for a “traffic impact fee,” even though, Sheetz alleged, there was no evidence the development would lead to more traffic.\u003c/p>\n\u003cp>On Friday, the U.S. Supreme Court ruled unanimously in favor of Sheetz, saying developers have a right to challenge the constitutionality of these fees. Though the case’s fate ultimately rests in a lower court, the high court’s ruling could mean more developers will take cities to court over what Sheetz argued was “extortionate fees.”\u003c/p>\n\u003cp>“The way impact fees have thus far been imposed has been arbitrary and varies widely from town to town,” Jim Wunderman, President and CEO of the Bay Area Council said in a \u003ca href=\"https://www.bayareacouncil.org/press-releases/bay-area-council-hails-supreme-court-decision-on-costly-impact-fees/\">statement\u003c/a>. The regional business advocacy organization was one of many to submit amicus briefs in favor of Sheetz’s case. “This ruling is hopefully the first step on the path to returning some fairness in how housing and other local impact fees are charged.”\u003c/p>\n\u003cp>Many cities, however, rely on these fees to fund government services and city maintenance. Jason Rhine, director of legislative affairs for the League of California Cities, argues impact fees simply account for more people living in a city once the new housing is built.\u003c/p>\n\u003cp>“Most cities do not have a lot of excess dollars lying around in their general fund to help subsidize these [new] projects,” he said. “Developers have to pay their fair share when it comes to the impact that project is going to have on their community.”\u003c/p>\n\u003cp>When voters in 1978 passed Proposition 13, which limits the amount cities can increase property taxes each year, this revenue accounted for 90% of a city’s total income. According to a \u003ca href=\"https://lao.ca.gov/Publications/Report/3497#How_Did_Proposition.A013_Change_Local_Governments_Mix_of_Tax_Revenues.3F\">study from the Legislative Analyst’s Office\u003c/a>, that share in 2016 was less than two-thirds.\u003c/p>\n\u003cp>“The biggest reason why impact fees are so pricey is due to municipal governments not having many ways to levy taxes,” said Muhammad Alameldin, a policy associate at UC Berkeley’s Terner Center for Housing Innovation.\u003c/p>\n\u003cp>Because Proposition 13 has artificially suppressed property tax revenue for decades, cities can no longer rely on property owners to foot the bill for maintaining their neighborhoods. Cities with fewer commercial centers, like San Jose or other suburban municipalities, are, therefore, in a tighter bind to find revenue.\u003c/p>\n\u003cp>Wiener said he was sympathetic to cities’ plight.\u003c/p>\n\u003cp>“We made it really hard for them to fund basic municipal services,” he said. “So, that’s why they have become overly reliant on impact fees on new housing.”\u003c/p>\n\u003cp>And he acknowledged that he and other lawmakers are kicking the can down the road on a much larger — and more meaningful — conversation.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"floatright"},"numeric":["floatright"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>“The much broader issue is how cities are funded in California,” Wiener said. “[My] bill is not a substitute for the broader conversation.”\u003c/p>\n\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983000/california-legislators-take-aim-at-construction-fees-to-boost-housing","authors":["11672"],"categories":["news_6266","news_8"],"tags":["news_32695","news_17620","news_1775","news_423"],"featImg":"news_11983025","label":"news"},"forum_2010101905411":{"type":"posts","id":"forum_2010101905411","meta":{"index":"posts_1591205157","site":"forum","id":"2010101905411","found":true},"guestAuthors":[],"slug":"bay-area-diaspora-closely-watching-indias-upcoming-election","title":"Bay Area Diaspora Closely Watching India’s Upcoming Election","publishDate":1713308077,"format":"audio","headTitle":"Bay Area Diaspora Closely Watching India’s Upcoming Election | KQED","labelTerm":{"site":"forum"},"content":"\u003cp>India’s general election will begin on Friday, as Prime Minister Narendra Modi seeks a third straight term in power. The election is set to be the biggest in history, with nearly a billion Indians eligible to cast ballots. Modi remains popular in India but has been criticized for his human rights record and attacks on the media and judiciary. We’ll preview the election, which runs through June, and hear from members of the Bay Area’s Indian communities.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\u003cp>\u003c/p>\n","blocks":[],"excerpt":"We’ll preview the election, which runs through June, and hear from members of the Bay Area’s Indian communities.","status":"publish","parent":0,"modified":1713379929,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":3,"wordCount":85},"headData":{"title":"Bay Area Diaspora Closely Watching India’s Upcoming Election | KQED","description":"We’ll preview the election, which runs through June, and hear from members of the Bay Area’s Indian communities.","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"audioUrl":"https://www.podtrac.com/pts/redirect.mp3/pdst.fm/e/chrt.fm/track/G6C7C3/traffic.megaphone.fm/KQINC4369739249.mp3?updated=1713379097","airdate":1713369600,"forumGuests":[{"name":"Anita Manwani","bio":"president, The Indus Entrepreneurs (TiE) Silicon Valley"},{"name":"Nikhil Inamdar","bio":"Indian business correspondent, BBC"},{"name":"Milan Vaishnav","bio":"senior fellow and director, South Asia Program at Carnegie Endowment for International Peace; host, Grand Tamasha podcast"},{"name":"Raju Rajagopal","bio":"co-founder, Hindus for Human Rights - He is based in Berkeley"}],"sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/forum/2010101905411/bay-area-diaspora-closely-watching-indias-upcoming-election","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>India’s general election will begin on Friday, as Prime Minister Narendra Modi seeks a third straight term in power. The election is set to be the biggest in history, with nearly a billion Indians eligible to cast ballots. Modi remains popular in India but has been criticized for his human rights record and attacks on the media and judiciary. We’ll preview the election, which runs through June, and hear from members of the Bay Area’s Indian communities.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\u003cp>\u003c/p>\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/forum/2010101905411/bay-area-diaspora-closely-watching-indias-upcoming-election","authors":["11757"],"categories":["forum_165"],"featImg":"forum_2010101905412","label":"forum"},"news_11983211":{"type":"posts","id":"news_11983211","meta":{"index":"posts_1591205157","site":"news","id":"11983211","found":true},"guestAuthors":[],"slug":"jail-deaths-prompt-calls-to-separate-coroner-and-sheriffs-departments-in-riverside-county","title":"Jail Deaths Prompt Calls To Separate Coroner And Sheriff's Departments In Riverside County","publishDate":1713362470,"format":"audio","headTitle":"Jail Deaths Prompt Calls To Separate Coroner And Sheriff’s Departments In Riverside County | KQED","labelTerm":{},"content":"\u003ch2>\u003cstrong>With Increase In In-Custody Deaths, Calls Grow For Sheriff To Separate From Coroner’s Job \u003c/strong>\u003c/h2>\n\u003cp>\u003cspan style=\"font-weight: 400\">In most California counties, the sheriff also oversees the coroner’s office. But in Riverside County, families whose loved ones have died in local jails say that’s a conflict of interest — and they want to change the system. \u003c/span>\u003cbr>\n\u003cem>\u003cspan style=\"font-weight: 400\">Reporter: Madison Aument, KVCR\u003c/span>\u003c/em>\u003c/p>\n\u003ch2>\u003cstrong>Momentum Building For National Monument Near Salton Sea\u003c/strong>\u003c/h2>\n\u003cp>\u003cspan style=\"font-weight: 400\">This week, US Senators Alex Padilla and Laphonza Butler announced legislation to create a new national monument on the north edge of the Salton Sea, east of Palm Springs. S\u003c/span>upporters say the land is especially important to communities of color.\u003cbr>\n\u003cem>\u003cspan style=\"font-weight: 400\">Reporter: Kori Suzuki, KPBS\u003c/span>\u003c/em>\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\u003cp>\u003c/p>\n","blocks":[],"excerpt":null,"status":"publish","parent":0,"modified":1713362470,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":4,"wordCount":118},"headData":{"title":"Jail Deaths Prompt Calls To Separate Coroner And Sheriff's Departments In Riverside County | KQED","description":"With Increase In In-Custody Deaths, Calls Grow For Sheriff To Separate From Coroner's Job In most California counties, the sheriff also oversees the coroner’s office. But in Riverside County, families whose loved ones have died in local jails say that's a conflict of interest — and they want to change the system. Reporter: Madison Aument, KVCR Momentum Building For National Monument Near Salton Sea This week, US Senators Alex Padilla and Laphonza Butler announced legislation to create a new national monument on the north edge of the Salton Sea, east of Palm Springs. Supporters say the land is especially important","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"source":"Morning Report","sourceUrl":"https://www.kqed.org/news/tag/tcrarchive/","audioUrl":"https://www.podtrac.com/pts/redirect.mp3/chrt.fm/track/G6C7C3/traffic.megaphone.fm/KQINC1571397038.mp3?updated=1713362374","sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/news/11983211/jail-deaths-prompt-calls-to-separate-coroner-and-sheriffs-departments-in-riverside-county","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003ch2>\u003cstrong>With Increase In In-Custody Deaths, Calls Grow For Sheriff To Separate From Coroner’s Job \u003c/strong>\u003c/h2>\n\u003cp>\u003cspan style=\"font-weight: 400\">In most California counties, the sheriff also oversees the coroner’s office. But in Riverside County, families whose loved ones have died in local jails say that’s a conflict of interest — and they want to change the system. \u003c/span>\u003cbr>\n\u003cem>\u003cspan style=\"font-weight: 400\">Reporter: Madison Aument, KVCR\u003c/span>\u003c/em>\u003c/p>\n\u003ch2>\u003cstrong>Momentum Building For National Monument Near Salton Sea\u003c/strong>\u003c/h2>\n\u003cp>\u003cspan style=\"font-weight: 400\">This week, US Senators Alex Padilla and Laphonza Butler announced legislation to create a new national monument on the north edge of the Salton Sea, east of Palm Springs. S\u003c/span>upporters say the land is especially important to communities of color.\u003cbr>\n\u003cem>\u003cspan style=\"font-weight: 400\">Reporter: Kori Suzuki, KPBS\u003c/span>\u003c/em>\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\u003cp>\u003c/p>\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983211/jail-deaths-prompt-calls-to-separate-coroner-and-sheriffs-departments-in-riverside-county","authors":["236"],"programs":["news_72"],"categories":["news_21291"],"tags":["news_21998","news_21268"],"featImg":"news_11983214","label":"source_news_11983211"},"news_11983285":{"type":"posts","id":"news_11983285","meta":{"index":"posts_1591205157","site":"news","id":"11983285","found":true},"guestAuthors":[],"slug":"federal-bureau-of-prisons-challenges-judges-decision-to-delay-inmate-transfers-from-fci-dublin","title":"Federal Bureau of Prisons Challenges Judge’s Order Delaying Inmate Transfers from FCI Dublin","publishDate":1713396565,"format":"standard","headTitle":"Federal Bureau of Prisons Challenges Judge’s Order Delaying Inmate Transfers from FCI Dublin | KQED","labelTerm":{"site":"news"},"content":"\u003cp>The Federal Bureau of Prisons is pushing back on a judge’s order delaying the mass transfer of hundreds of incarcerated women at FCI Dublin, days after the agency’s director publicly announced it was shutting down the prison.\u003c/p>\n\u003cp>In a brief filed Tuesday, government attorneys said the court’s order, as well as the interpretation of that order by the recently appointed special master, have significantly delayed the transfer of women to other facilities.\u003c/p>\n\u003cp>“The logistical details involved with the mass transfer of all [incarcerated people] at a particular facility cannot be changed on the fly,” the government’s brief reads. “Extensive resources and employee hours have already been invested in the move.”\u003c/p>\n\u003cp>\u003cb>Catch up fast: \u003c/b>\u003ca href=\"https://www.kqed.org/news/11983151/infamous-womens-prison-plagued-by-sex-abuse-closes\">The federal Bureau of Prisons announced Monday it would close FCI Dublin\u003c/a> after years of staff sexual misconduct allegations, multiple criminal indictments and dozens of lawsuits alleging sexual assault, harassment and retaliation.\u003c/p>\n\u003cp>In a statement, BOP Director Colette S. Peters said that the agency had provided tremendous resources to address the culture at FCI Dublin. “Despite these steps and resources, we have determined that FCI Dublin is not meeting expected standards and that the best course of action is to close the facility,” she added.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>[aside postID=\"news_11979936,news_11980960,news_11978878\" label=\"Related Stories\"]Within hours of the announcement, U.S. District Judge Yvonne Gonzalez Rogers issued an order requiring prison officials to update casework for all inmates to ensure they are sent to the correct location — another BOP facility, home confinement or a halfway house, or if they should be granted compassionate release. “The result of these case reviews and transfer designations shall be reviewed with the Special Master prior to transfer,” the order reads. Another document detailing additional guidance to BOP on the transfers was filed under seal.\u003c/p>\n\u003cp>In the Tuesday brief, government attorneys wrote that the special master, Wendy Still, had told FCI Dublin’s interim warden, Nancy McKinney, that she interpreted the court’s order as authorizing her to have each incarcerated person medically reviewed by her staff and a BOP doctor before approving the transfer. “These procedures — above what BOP requires — are significantly delaying the transfer process,” attorneys wrote, arguing that the court does not have the authority to decide when inmates in its custody should be transferred.\u003c/p>\n\u003cp>“It is beyond question that transfer of inmates falls within the exclusive authority of the BOP, and it is not subject to judicial review,” the brief reads.\u003c/p>\n\u003cp>\u003cb>How many people have been transferred so far?\u003c/b> It’s unclear. A BOP spokesperson declined to comment beyond Peters’ initial statement on the closure — which said the timing of transfers would not be shared — citing “safety and security reasons.”\u003c/p>\n\u003cp>In an interview with KQED on Tuesday, an incarcerated woman described a chaotic scene at the prison as officials attempted to transfer roughly 600 or so people.\u003c/p>\n\u003cp>Ashley Castillo said she and other prisoners learned about the closure on Monday morning through news reports. They were subsequently told 100 people would be transferred per day, with the first group of prisoners — including Castillo — leaving that same day. As the women were given a green bag to fill with their belongings, they noticed officers from other BOP facilities had replaced the prison’s usual staff, Castillo said. Some women got on a bus to leave but ultimately returned to the prison, she added.\u003c/p>\n\u003cp>“They packed people out and they even dressed them out, and they let them board the bus,” Castillo said. “And then at the end, like around three o’clock, they brought them back. They dressed them out again, gave them their uniforms again, and they said you guys are not going nowhere.”\u003c/p>\n\u003cp>Still, who Gonzalez Rogers appointed barely a week and a half ago, and is tasked with overseeing a series of reforms at FCI Dublin, was at the prison on Monday and Tuesday communicating with prisoners, according to Castillo.\u003c/p>\n\u003cp>“We were all going crazy not knowing what was going on. [Still] said, ‘Don’t worry, I’m talking to the judge right now, and I’m trying to put a stop to it because you guys are not medically cleared to go anywhere,’” Castillo recalled, adding that the uncertainty of the announcement had created confusion and distress among women at the prison who were frantically trying to get ahold of their families.\u003c/p>\n\u003cp>\u003cb>The latest: \u003c/b>Two hearings were held this morning that were closed to the public. Shortly after, Gonzalez Rogers issued another order, under seal, with further guidance on the transfers. Attorneys representing women in the class-action lawsuit did not respond to a request for comment on hearings held this morning.\u003c/p>\n\u003cp>Castillo’s attorney, Alana McMains, told KQED she received emails from both of her clients at FCI Dublin saying they expected to be transferred on Wednesday.\u003c/p>\n\u003cp>“I have no idea if they actually got a chance to meet the special master and inquire about compassionate release,” McMains said.\u003c/p>\n\u003cp>\u003cb>How did we get here?: \u003c/b>In March, FBI agents raided FCI Dublin. BOP announced it was replacing core members of the prison’s leadership staff hours later.\u003c/p>\n\u003cul>\n\u003cli style=\"font-weight: 400\">Several days later, Gonzalez Rogers ordered the appointment of a special master, an independent third party, to oversee immediate changes at the facility.\u003c/li>\n\u003cli style=\"font-weight: 400\">Still, the former chief probation officer for Alameda and San Francisco counties was appointed special master on April 5. Still and her staff were given full access to the prison and its records.\u003c/li>\n\u003cli style=\"font-weight: 400\">According to an attorney representing incarcerated women in a class action lawsuit, Still was at FCI Dublin the following April 8 and at least one other time that week.\u003c/li>\n\u003cli style=\"font-weight: 400\">On April 15, BOP announced it was closing FCI Dublin.\u003c/li>\n\u003c/ul>\n\u003cp>\u003cb>What’s next: \u003c/b>On Thursday, Darrell Wayne Smith, the last FCI Dublin officer facing criminal charges for alleged sex abuse, is scheduled for a status conference.\u003c/p>\n\u003cp>Smith was arrested in May 2023 and charged with five counts of sexual abuse of a prisoner, six counts of abusive sexual contact and one count of aggravated sexual abuse. An indictment describes 12 incidents between May 2019 and May 2021, during which Smith allegedly had sexual contact with three women incarcerated at the prison.\u003c/p>\n\u003cp>[ad floatright]\u003c/p>\n\u003cp>Earlier this month, Smith’s attorneys filed a motion to withdraw themselves from his case, saying that his financial circumstances had significantly changed and that he could no longer afford private counsel.\u003c/p>\n\n","blocks":[],"excerpt":"The Federal Bureau of Prisons is pushing back on a judge’s order delaying the mass transfer of hundreds of incarcerated women at FCI Dublin, days after the agency’s director publicly announced it was shutting down the prison. ","status":"publish","parent":0,"modified":1713398589,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":23,"wordCount":1105},"headData":{"title":"Federal Bureau of Prisons Challenges Judge’s Order Delaying Inmate Transfers from FCI Dublin | KQED","description":"The Federal Bureau of Prisons is pushing back on a judge’s order delaying the mass transfer of hundreds of incarcerated women at FCI Dublin, days after the agency’s director publicly announced it was shutting down the prison. ","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":""},"sticky":false,"excludeFromSiteSearch":"Include","articleAge":"0","path":"/news/11983285/federal-bureau-of-prisons-challenges-judges-decision-to-delay-inmate-transfers-from-fci-dublin","audioTrackLength":null,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>The Federal Bureau of Prisons is pushing back on a judge’s order delaying the mass transfer of hundreds of incarcerated women at FCI Dublin, days after the agency’s director publicly announced it was shutting down the prison.\u003c/p>\n\u003cp>In a brief filed Tuesday, government attorneys said the court’s order, as well as the interpretation of that order by the recently appointed special master, have significantly delayed the transfer of women to other facilities.\u003c/p>\n\u003cp>“The logistical details involved with the mass transfer of all [incarcerated people] at a particular facility cannot be changed on the fly,” the government’s brief reads. “Extensive resources and employee hours have already been invested in the move.”\u003c/p>\n\u003cp>\u003cb>Catch up fast: \u003c/b>\u003ca href=\"https://www.kqed.org/news/11983151/infamous-womens-prison-plagued-by-sex-abuse-closes\">The federal Bureau of Prisons announced Monday it would close FCI Dublin\u003c/a> after years of staff sexual misconduct allegations, multiple criminal indictments and dozens of lawsuits alleging sexual assault, harassment and retaliation.\u003c/p>\n\u003cp>In a statement, BOP Director Colette S. Peters said that the agency had provided tremendous resources to address the culture at FCI Dublin. “Despite these steps and resources, we have determined that FCI Dublin is not meeting expected standards and that the best course of action is to close the facility,” she added.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"postid":"news_11979936,news_11980960,news_11978878","label":"Related Stories "},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>Within hours of the announcement, U.S. District Judge Yvonne Gonzalez Rogers issued an order requiring prison officials to update casework for all inmates to ensure they are sent to the correct location — another BOP facility, home confinement or a halfway house, or if they should be granted compassionate release. “The result of these case reviews and transfer designations shall be reviewed with the Special Master prior to transfer,” the order reads. Another document detailing additional guidance to BOP on the transfers was filed under seal.\u003c/p>\n\u003cp>In the Tuesday brief, government attorneys wrote that the special master, Wendy Still, had told FCI Dublin’s interim warden, Nancy McKinney, that she interpreted the court’s order as authorizing her to have each incarcerated person medically reviewed by her staff and a BOP doctor before approving the transfer. “These procedures — above what BOP requires — are significantly delaying the transfer process,” attorneys wrote, arguing that the court does not have the authority to decide when inmates in its custody should be transferred.\u003c/p>\n\u003cp>“It is beyond question that transfer of inmates falls within the exclusive authority of the BOP, and it is not subject to judicial review,” the brief reads.\u003c/p>\n\u003cp>\u003cb>How many people have been transferred so far?\u003c/b> It’s unclear. A BOP spokesperson declined to comment beyond Peters’ initial statement on the closure — which said the timing of transfers would not be shared — citing “safety and security reasons.”\u003c/p>\n\u003cp>In an interview with KQED on Tuesday, an incarcerated woman described a chaotic scene at the prison as officials attempted to transfer roughly 600 or so people.\u003c/p>\n\u003cp>Ashley Castillo said she and other prisoners learned about the closure on Monday morning through news reports. They were subsequently told 100 people would be transferred per day, with the first group of prisoners — including Castillo — leaving that same day. As the women were given a green bag to fill with their belongings, they noticed officers from other BOP facilities had replaced the prison’s usual staff, Castillo said. Some women got on a bus to leave but ultimately returned to the prison, she added.\u003c/p>\n\u003cp>“They packed people out and they even dressed them out, and they let them board the bus,” Castillo said. “And then at the end, like around three o’clock, they brought them back. They dressed them out again, gave them their uniforms again, and they said you guys are not going nowhere.”\u003c/p>\n\u003cp>Still, who Gonzalez Rogers appointed barely a week and a half ago, and is tasked with overseeing a series of reforms at FCI Dublin, was at the prison on Monday and Tuesday communicating with prisoners, according to Castillo.\u003c/p>\n\u003cp>“We were all going crazy not knowing what was going on. [Still] said, ‘Don’t worry, I’m talking to the judge right now, and I’m trying to put a stop to it because you guys are not medically cleared to go anywhere,’” Castillo recalled, adding that the uncertainty of the announcement had created confusion and distress among women at the prison who were frantically trying to get ahold of their families.\u003c/p>\n\u003cp>\u003cb>The latest: \u003c/b>Two hearings were held this morning that were closed to the public. Shortly after, Gonzalez Rogers issued another order, under seal, with further guidance on the transfers. Attorneys representing women in the class-action lawsuit did not respond to a request for comment on hearings held this morning.\u003c/p>\n\u003cp>Castillo’s attorney, Alana McMains, told KQED she received emails from both of her clients at FCI Dublin saying they expected to be transferred on Wednesday.\u003c/p>\n\u003cp>“I have no idea if they actually got a chance to meet the special master and inquire about compassionate release,” McMains said.\u003c/p>\n\u003cp>\u003cb>How did we get here?: \u003c/b>In March, FBI agents raided FCI Dublin. BOP announced it was replacing core members of the prison’s leadership staff hours later.\u003c/p>\n\u003cul>\n\u003cli style=\"font-weight: 400\">Several days later, Gonzalez Rogers ordered the appointment of a special master, an independent third party, to oversee immediate changes at the facility.\u003c/li>\n\u003cli style=\"font-weight: 400\">Still, the former chief probation officer for Alameda and San Francisco counties was appointed special master on April 5. Still and her staff were given full access to the prison and its records.\u003c/li>\n\u003cli style=\"font-weight: 400\">According to an attorney representing incarcerated women in a class action lawsuit, Still was at FCI Dublin the following April 8 and at least one other time that week.\u003c/li>\n\u003cli style=\"font-weight: 400\">On April 15, BOP announced it was closing FCI Dublin.\u003c/li>\n\u003c/ul>\n\u003cp>\u003cb>What’s next: \u003c/b>On Thursday, Darrell Wayne Smith, the last FCI Dublin officer facing criminal charges for alleged sex abuse, is scheduled for a status conference.\u003c/p>\n\u003cp>Smith was arrested in May 2023 and charged with five counts of sexual abuse of a prisoner, six counts of abusive sexual contact and one count of aggravated sexual abuse. An indictment describes 12 incidents between May 2019 and May 2021, during which Smith allegedly had sexual contact with three women incarcerated at the prison.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"floatright"},"numeric":["floatright"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>Earlier this month, Smith’s attorneys filed a motion to withdraw themselves from his case, saying that his financial circumstances had significantly changed and that he could no longer afford private counsel.\u003c/p>\n\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11983285/federal-bureau-of-prisons-challenges-judges-decision-to-delay-inmate-transfers-from-fci-dublin","authors":["11490"],"categories":["news_8"],"tags":["news_32222","news_27626","news_33888"],"featImg":"news_11983294","label":"news"},"news_11728856":{"type":"posts","id":"news_11728856","meta":{"index":"posts_1591205157","site":"news","id":"11728856","found":true},"guestAuthors":[],"slug":"stanford-researchers-using-mri-scans-to-predict-meth-and-cocaine-relapse","title":"Stanford Researchers Using MRI Scans to Predict Meth and Cocaine Relapse","publishDate":1551224445,"format":"audio","headTitle":"The California Report | KQED News","labelTerm":{"term":72,"site":"news"},"content":"\u003cp>Dee Dee is lying on her back, the cacophony of the MRI machine’s ringing and buzzing all around her head.\u003c/p>\n\u003cp>She stares straight up at a mirror that’s tilted so she can see a computer screen at her feet. It projects a series of images: a glass of beer, a piece of pizza, a line of methamphetamine. In her hands, she holds the controls to indicate, on a scale of 1 to 4, how much she wants what’s in the picture.\u003c/p>\n\u003cp>The more detailed the photos became, the more she wanted what was in them, she said later. A bag of white powder? No big deal. But a needle, with speed in it, ready to inject? That was different.\u003c/p>\n\u003cp>“The interest went from, ‘No? No.’ To just all of a sudden, ‘Yeah, yeah, yeah,’ ” she says. “Just thinking about it right now, I can kind of taste it in the back of my throat.”\u003c/p>\n\u003cp>A team of researchers at Stanford University are scanning the brains of stimulant users like Dee Dee to better understand one of the most intractable and frustrating questions in addiction treatment: Who is most likely to relapse and why? Current studies show that \u003ca href=\"https://www.sciencedirect.com/science/article/pii/S0376871614007728?via%3Dihub\" target=\"_blank\" rel=\"noopener\">60 percent of people\u003c/a> in rehab for meth addiction relapse within a year of discharge, a stat that has health officials on edge as meth use in San Francisco is \u003ca href=\"https://www.kqed.org/news/11724407/meths-comeback-a-new-speed-epidemic-takes-its-toll-on-san-francisco\" target=\"_blank\" rel=\"noopener\">again surging\u003c/a>.\u003c/p>\n\u003cp>[ad fullwidth]\u003c/p>\n\u003cp>Neuropsychologist Kelly MacNiven and her team believe they may have identified a signal in the brain that can predict who will relapse.\u003c/p>\n\u003cp>“We can potentially use this to see who is at greater risk for relapse,” MacNiven says. “We can also potentially try to develop better interventions that target this brain activity, and we can see if by reducing this brain activity, if that can reduce relapse risk.”\u003c/p>\n\u003cfigure id=\"attachment_11728945\" class=\"wp-caption aligncenter\" style=\"max-width: 800px\">\u003cimg class=\"size-medium wp-image-11728945\" src=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/Kelly-MacNiven-2-800x600.jpg\" alt=\"\" width=\"800\" height=\"600\">\u003cfigcaption class=\"wp-caption-text\">Neuropsychologist Kelly MacNiven sets up the MRI scanner at Stanford. \u003ccite>(April Dembosky/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>While test subjects like Dee Dee look at pictures in the MRI scanner, MacNiven sits on the other side of the wall, looking at the brain scans on her computer screen. When all the scans are complete, the teams goes over them, specifically studying the nucleus accumbens, located in the middle of the brain.\u003c/p>\n\u003cp>In their \u003ca href=\"https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2719577\" target=\"_blank\" rel=\"noopener\">first round\u003c/a> of the scanning study, MacNiven’s team found that the people whose brains really light up in this spot when they’re looking at the pictures of meth and cocaine are the ones most likely to relapse. Six months after the scan, they were twice as likely to have used again.\u003c/p>\n\u003cp>“This suggests, if this replicates, that we have a brain signal that basically is related to relapse,” says MacNiven, a postdoc fellow in the psychology department at Stanford and lead author of the study.\u003c/p>\n\u003cp>\u003cstrong>Confronting Relapse\u003c/strong>\u003c/p>\n\u003cp>Dee Dee was 14 when she tried methamphetamine for the first time. Her parents had recently gotten divorced.\u003c/p>\n\u003cp>“My family, in the blink of an eye, was torn apart and I didn’t understand it,” says Dee Dee, who asked that we not reveal her last name. “I remember just being really broken.\"\u003c/p>\n\u003cp>She had to move, and the kids she became friends with were experimenting with all kinds of drugs. But she liked meth the best.\u003c/p>\n\u003cp>“When I smoked pot, it made me hungry and it just made me really tired. Meth was the total opposite, I had energy,” she says. “Me and my friends, we went from like not wanting to do anything to just like wanting to clean, and like, kind of like you feel like you're being productive.”\u003c/p>\n\u003cp>[aside hero=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/GettyImages-458902784.jpg\" label=\"Meth's Comeback\" link1=\"https://www.kqed.org/news/11724407/meths-comeback-a-new-speed-epidemic-takes-its-toll-on-san-francisco,Meth's Comeback: A New Speed Epidemic Takes Its Toll on San Francisco\" link2=\"https://www.kqed.org/news/11728012/lack-of-medication-treatments-for-meth-frustrates-doctors,Lack of Medication Treatments for Meth Frustrates Doctors\"]\u003c/p>\n\u003cp>She used on and off for years, then went into treatment when she was 26. She met a guy there. They got sober together and had a baby. Then he relapsed. And then Dee Dee relapsed. She was using meth every day.\u003c/p>\n\u003cp>“My line of work was high sales, so I had to always have my A-game on,” she says. “Even when I was really tired from being a young mom, it gave me energy to do everything.”\u003c/p>\n\u003cp>Within four months, Dee Dee lost her job, her apartment, her car. Now she’s in treatment again, trying to understand what it was about last time that didn’t stick.\u003c/p>\n\u003cp>“I just don’t want to be in and out of treatment centers. I want to get it right,” she says.\u003c/p>\n\u003cp>\u003cstrong>Dopamine Versus Self-report\u003c/strong>\u003c/p>\n\u003cp>Relapse most often results from a trigger in the user’s environment: driving past the bar they used to go to in order to get high, the smell of a certain cigarette or running into someone they used to use with.\u003c/p>\n\u003cp>This is what researchers are trying to emulate in the MRI lab, by showing pictures of drug paraphernalia to elicit the same response in the brain.\u003c/p>\n\u003cp>MacNiven and her team believe dopamine is at work here: Before a person has smoked or snorted any drug, the brain releases a bit of dopamine in anticipation of getting high.\u003c/p>\n\u003cp>“Addictive drugs are in some way hijacking the dopamine system,” MacNiven says.\u003c/p>\n\u003cp>They do this in two ways. First, there’s the dopamine response to the meth itself that makes a person feel really, really good. Second, there’s a kind of learned behavior, a trained dopamine release at the sight of the meth, or the old bar or friend — this is the brain teaching itself what behaviors lead to the ingestion of the drug that feels so good.\u003c/p>\n\u003cfigure id=\"attachment_11728944\" class=\"wp-caption aligncenter\" style=\"max-width: 800px\">\u003cimg class=\"size-medium wp-image-11728944\" src=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/Nucleus-accumbens-800x600.jpg\" alt=\"\" width=\"800\" height=\"600\">\u003cfigcaption class=\"wp-caption-text\">MacNiven points to the nucleus accumbens. People who showed the most activity in this part of the brain while looking at images of drugs were the most likely to relapse. \u003ccite>(April Dembosky/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>In animal studies, this anticipatory dopamine release goes straight to the nucleus accumbens in the middle of the brain. The \u003ca href=\"https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2719577\" target=\"_blank\" rel=\"noopener\">Stanford study\u003c/a> is the first to replicate this in humans.\u003c/p>\n\u003cp>They believe this brain marker is a much more robust, dependable predictor of who will relapse, as opposed to users reporting cravings or environmental triggers. The study showed that users themselves cannot predict their own likelihood of relapse.\u003c/p>\n\u003cp>So even though Dee Dee could taste drugs in the back of her throat when thinking about pictures of dope, in the end, that may have no bearing on her risk of relapse. In MacNiven’s first round of tests, what former drug users said they wanted had no relation to what their brains said they wanted, MacNiven says. Self-reports did not predict who ended up relapsing and who didn’t. Only the brain activity did.\u003c/p>\n\u003cp>“We actually think this is interesting and might be a factor related to addiction, meaning that you might not have the ability to really know what you want,” MacNiven says.\u003c/p>\n\u003cp>To be sure of this conclusion, researchers have to test more people. They did the first round of scans on veterans — almost all men. Historically, this is true of a lot of addiction research. MacNiven is now actively recruiting and testing women to make sure her results hold up.\u003c/p>\n\u003cp>“This confirmation is vital, as women with stimulant use disorders may have more intense craving after drug cessation,” wrote Jay Nierenberg, a psychiatry professor at NYU School of Medicine, in \u003ca href=\"https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2719570\" target=\"_blank\" rel=\"noopener\">a paper\u003c/a> reviewing the Stanford results among vets. “And poorer clinical outcomes among women with stimulant use disorders have been reported in multiple studies.”\u003c/p>\n\u003cfigure id=\"attachment_11728951\" class=\"wp-caption aligncenter\" style=\"max-width: 800px\">\u003cimg class=\"size-medium wp-image-11728951\" src=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/Needle-and-spoon-800x600.jpg\" alt=\"\" width=\"800\" height=\"600\">\u003cfigcaption class=\"wp-caption-text\">What former users said they wanted had no bearing on whether they went on to relapse. \u003ccite>(April Dembosky/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>\u003cstrong>Implications for Treatment\u003c/strong>\u003c/p>\n\u003cp>If the findings do hold up in a larger, more diverse population, the implications could be powerful. Treatment providers could tailor care more specifically and target more precisely who should get what kind of treatment and for how long.\u003c/p>\n\u003cp>“Identifying those at greatest risk and providing treatment that specifically targets modifiable components of that risk would undoubtedly change the landscape of substance abuse treatment, likely attracting more people who need it and perhaps reducing burnout among those who provide it,” Nierenberg writes.\u003c/p>\n\u003cp>But it also means the only way to know who’s at highest risk for relapse requires giving everyone an MRI.\u003c/p>\n\u003cp>“I would say, is that so bad?” MacNiven asks. “Doing a $400 MRI scan, if that actually keeps people from relapsing, then I would say that it’s worth it.”\u003c/p>\n\u003cp>But of course getting access to this kind of diagnostic care is much more complicated than that. Not everyone who needs help with relapse lives near Stanford, or any MRI lab, and the details of this experiment are complex and difficult to emulate in other clinical settings. Plus, the scans take six hours for each test subject — not everyone can tolerate being enclosed in a tight, noisy machine for that long.\u003c/p>\n\u003cp>\"These results help to advance the field, although use in clinical practice is unlikely, at least for the time being,\" says Dr. Phillip Coffin, director of substance use research at the San Francisco Department of Public Health.\u003c/p>\n\u003cp>Then there is the question of effective treatments. There are no Food and Drug Administration-approved \u003ca href=\"https://www.kqed.org/news/11728012/lack-of-medication-treatments-for-meth-frustrates-doctors\" target=\"_blank\" rel=\"noopener\">medications for stimulant addiction\u003c/a> the way there are for opioids.\u003c/p>\n\u003cp>MacNiven and her team are brainstorming other options from their research — things like magnetic stimulation of the scalp to interfere with the brain’s addiction activity. Or neurofeedback, where users train their own brains not to light up at the sight of drugs.\u003c/p>\n\u003cp>“The idea that there could be anything that is an option for people, that is not the conventional standard stuff, is really exciting to people,” MacNiven says, “even if it’s something like brain zapping.”\u003c/p>\n\u003cp>That would be a relief to folks like Dee Dee. She’s been in treatment for four months so far at the \u003ca href=\"https://www.theepiphanycenter.org/\" target=\"_blank\" rel=\"noopener\">Epiphany Center\u003c/a>, a residential program for women in San Francisco. She admits her initial interest in participating in the study was for the free lunch and the Amazon gift card. But that changed the more she understood the research goals.\u003c/p>\n\u003cp>[ad floatright]\u003c/p>\n\u003cp>“Anything that I can use to help people understand why we do the things we do, or maybe help someone to say no to drugs?” she says, “I'm all for it.”\u003c/p>\n\n","blocks":[],"excerpt":"A team of researchers at Stanford are scanning the brains of stimulant users to better understand one of the most intractable and frustrating questions in addiction treatment: Who is most likely to relapse and why?","status":"publish","parent":0,"modified":1551224445,"stats":{"hasAudio":false,"hasVideo":false,"hasChartOrMap":false,"iframeSrcs":[],"hasGoogleForm":false,"hasGallery":false,"hasHearkenModule":false,"hasPolis":false,"paragraphCount":46,"wordCount":1828},"headData":{"title":"Stanford Researchers Using MRI Scans to Predict Meth and Cocaine Relapse | KQED","description":"A team of researchers at Stanford are scanning the brains of stimulant users to better understand one of the most intractable and frustrating questions in addiction treatment: Who is most likely to relapse and why?","ogTitle":"","ogDescription":"","ogImgId":"","twTitle":"","twDescription":"","twImgId":"","authorsData":[{"type":"authors","id":"3205","meta":{"index":"authors_1591205172","id":"3205","found":true},"name":"April Dembosky","firstName":"April","lastName":"Dembosky","slug":"adembosky","email":"adembosky@kqed.org","display_author_email":false,"staff_mastheads":["news","science"],"title":"KQED Health Correspondent","bio":"April Dembosky is the health correspondent for KQED News and a regular contributor to NPR. She specializes in covering altered states of mind, from postpartum depression to methamphetamine-induced psychosis to the insanity defense. Her investigative series on insurance companies sidestepping mental health laws won multiple awards, including first place in beat reporting from the national Association of Health Care Journalists. She is the recipient of numerous other prizes and fellowships, including a national Edward R. Murrow award for investigative reporting, a Society of Professional Journalists award for long-form storytelling, and a Carter Center Fellowship for Mental Health Journalism.\r\n\r\nDembosky reported and produced \u003cem>Soundtrack of Silence\u003c/em>, an audio documentary about music and memory that is currently being made into a feature film by Paramount Pictures.\r\n\r\nBefore joining KQED in 2013, Dembosky covered technology and Silicon Valley for \u003cem>The Financial Times of London,\u003c/em> and contributed business and arts stories to \u003cem>Marketplace \u003c/em>and \u003cem>The New York Times.\u003c/em> She got her undergraduate degree in philosophy from Smith College and her master's in journalism from the University of California, Berkeley. She is a classically trained violinist and proud alum of the first symphony orchestra at Burning Man.","avatar":"https://secure.gravatar.com/avatar/ef92999be4ceb9ea60701e7dc276f813?s=600&d=blank&r=g","twitter":"adembosky","facebook":null,"instagram":null,"linkedin":null,"sites":[{"site":"arts","roles":["author"]},{"site":"news","roles":["editor"]},{"site":"futureofyou","roles":["author"]},{"site":"stateofhealth","roles":["editor"]},{"site":"science","roles":["editor"]},{"site":"forum","roles":["editor"]}],"headData":{"title":"April Dembosky | KQED","description":"KQED Health Correspondent","ogImgSrc":"https://secure.gravatar.com/avatar/ef92999be4ceb9ea60701e7dc276f813?s=600&d=blank&r=g","twImgSrc":"https://secure.gravatar.com/avatar/ef92999be4ceb9ea60701e7dc276f813?s=600&d=blank&r=g"},"isLoading":false,"link":"/author/adembosky"}],"imageData":{"ogImageSize":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-1020x765.jpg","width":1020,"height":765,"mimeType":"image/jpeg"},"twImageSize":{"file":"https://ww2.kqed.org/app/uploads/sites/10/2019/02/Stanford-study-coke-1020x765.jpg","width":1020,"height":765,"mimeType":"image/jpeg"},"twitterCard":"summary_large_image"},"tagData":{"tags":["addiction","meth","methamphetamine"]}},"disqusIdentifier":"11728856 https://ww2.kqed.org/news/?p=11728856","disqusUrl":"https://ww2.kqed.org/news/2019/02/26/stanford-researchers-using-mri-scans-to-predict-meth-and-cocaine-relapse/","disqusTitle":"Stanford Researchers Using MRI Scans to Predict Meth and Cocaine Relapse","audioUrl":"https://www.kqed.org/.stream/anon/radio/RDnews/2019/02/DemboskyMethTreatment.mp3","audioTrackLength":360,"path":"/news/11728856/stanford-researchers-using-mri-scans-to-predict-meth-and-cocaine-relapse","audioDuration":376000,"parsedContent":[{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003cp>Dee Dee is lying on her back, the cacophony of the MRI machine’s ringing and buzzing all around her head.\u003c/p>\n\u003cp>She stares straight up at a mirror that’s tilted so she can see a computer screen at her feet. It projects a series of images: a glass of beer, a piece of pizza, a line of methamphetamine. In her hands, she holds the controls to indicate, on a scale of 1 to 4, how much she wants what’s in the picture.\u003c/p>\n\u003cp>The more detailed the photos became, the more she wanted what was in them, she said later. A bag of white powder? No big deal. But a needle, with speed in it, ready to inject? That was different.\u003c/p>\n\u003cp>“The interest went from, ‘No? No.’ To just all of a sudden, ‘Yeah, yeah, yeah,’ ” she says. “Just thinking about it right now, I can kind of taste it in the back of my throat.”\u003c/p>\n\u003cp>A team of researchers at Stanford University are scanning the brains of stimulant users like Dee Dee to better understand one of the most intractable and frustrating questions in addiction treatment: Who is most likely to relapse and why? Current studies show that \u003ca href=\"https://www.sciencedirect.com/science/article/pii/S0376871614007728?via%3Dihub\" target=\"_blank\" rel=\"noopener\">60 percent of people\u003c/a> in rehab for meth addiction relapse within a year of discharge, a stat that has health officials on edge as meth use in San Francisco is \u003ca href=\"https://www.kqed.org/news/11724407/meths-comeback-a-new-speed-epidemic-takes-its-toll-on-san-francisco\" target=\"_blank\" rel=\"noopener\">again surging\u003c/a>.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"fullwidth"},"numeric":["fullwidth"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>Neuropsychologist Kelly MacNiven and her team believe they may have identified a signal in the brain that can predict who will relapse.\u003c/p>\n\u003cp>“We can potentially use this to see who is at greater risk for relapse,” MacNiven says. “We can also potentially try to develop better interventions that target this brain activity, and we can see if by reducing this brain activity, if that can reduce relapse risk.”\u003c/p>\n\u003cfigure id=\"attachment_11728945\" class=\"wp-caption aligncenter\" style=\"max-width: 800px\">\u003cimg class=\"size-medium wp-image-11728945\" src=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/Kelly-MacNiven-2-800x600.jpg\" alt=\"\" width=\"800\" height=\"600\">\u003cfigcaption class=\"wp-caption-text\">Neuropsychologist Kelly MacNiven sets up the MRI scanner at Stanford. \u003ccite>(April Dembosky/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>While test subjects like Dee Dee look at pictures in the MRI scanner, MacNiven sits on the other side of the wall, looking at the brain scans on her computer screen. When all the scans are complete, the teams goes over them, specifically studying the nucleus accumbens, located in the middle of the brain.\u003c/p>\n\u003cp>In their \u003ca href=\"https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2719577\" target=\"_blank\" rel=\"noopener\">first round\u003c/a> of the scanning study, MacNiven’s team found that the people whose brains really light up in this spot when they’re looking at the pictures of meth and cocaine are the ones most likely to relapse. Six months after the scan, they were twice as likely to have used again.\u003c/p>\n\u003cp>“This suggests, if this replicates, that we have a brain signal that basically is related to relapse,” says MacNiven, a postdoc fellow in the psychology department at Stanford and lead author of the study.\u003c/p>\n\u003cp>\u003cstrong>Confronting Relapse\u003c/strong>\u003c/p>\n\u003cp>Dee Dee was 14 when she tried methamphetamine for the first time. Her parents had recently gotten divorced.\u003c/p>\n\u003cp>“My family, in the blink of an eye, was torn apart and I didn’t understand it,” says Dee Dee, who asked that we not reveal her last name. “I remember just being really broken.\"\u003c/p>\n\u003cp>She had to move, and the kids she became friends with were experimenting with all kinds of drugs. But she liked meth the best.\u003c/p>\n\u003cp>“When I smoked pot, it made me hungry and it just made me really tired. Meth was the total opposite, I had energy,” she says. “Me and my friends, we went from like not wanting to do anything to just like wanting to clean, and like, kind of like you feel like you're being productive.”\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"aside","attributes":{"named":{"hero":"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/GettyImages-458902784.jpg","label":"Meth's Comeback ","link1":"https://www.kqed.org/news/11724407/meths-comeback-a-new-speed-epidemic-takes-its-toll-on-san-francisco,Meth's Comeback: A New Speed Epidemic Takes Its Toll on San Francisco","link2":"https://www.kqed.org/news/11728012/lack-of-medication-treatments-for-meth-frustrates-doctors,Lack of Medication Treatments for Meth Frustrates Doctors"},"numeric":[]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>She used on and off for years, then went into treatment when she was 26. She met a guy there. They got sober together and had a baby. Then he relapsed. And then Dee Dee relapsed. She was using meth every day.\u003c/p>\n\u003cp>“My line of work was high sales, so I had to always have my A-game on,” she says. “Even when I was really tired from being a young mom, it gave me energy to do everything.”\u003c/p>\n\u003cp>Within four months, Dee Dee lost her job, her apartment, her car. Now she’s in treatment again, trying to understand what it was about last time that didn’t stick.\u003c/p>\n\u003cp>“I just don’t want to be in and out of treatment centers. I want to get it right,” she says.\u003c/p>\n\u003cp>\u003cstrong>Dopamine Versus Self-report\u003c/strong>\u003c/p>\n\u003cp>Relapse most often results from a trigger in the user’s environment: driving past the bar they used to go to in order to get high, the smell of a certain cigarette or running into someone they used to use with.\u003c/p>\n\u003cp>This is what researchers are trying to emulate in the MRI lab, by showing pictures of drug paraphernalia to elicit the same response in the brain.\u003c/p>\n\u003cp>MacNiven and her team believe dopamine is at work here: Before a person has smoked or snorted any drug, the brain releases a bit of dopamine in anticipation of getting high.\u003c/p>\n\u003cp>“Addictive drugs are in some way hijacking the dopamine system,” MacNiven says.\u003c/p>\n\u003cp>They do this in two ways. First, there’s the dopamine response to the meth itself that makes a person feel really, really good. Second, there’s a kind of learned behavior, a trained dopamine release at the sight of the meth, or the old bar or friend — this is the brain teaching itself what behaviors lead to the ingestion of the drug that feels so good.\u003c/p>\n\u003cfigure id=\"attachment_11728944\" class=\"wp-caption aligncenter\" style=\"max-width: 800px\">\u003cimg class=\"size-medium wp-image-11728944\" src=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/Nucleus-accumbens-800x600.jpg\" alt=\"\" width=\"800\" height=\"600\">\u003cfigcaption class=\"wp-caption-text\">MacNiven points to the nucleus accumbens. People who showed the most activity in this part of the brain while looking at images of drugs were the most likely to relapse. \u003ccite>(April Dembosky/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>In animal studies, this anticipatory dopamine release goes straight to the nucleus accumbens in the middle of the brain. The \u003ca href=\"https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2719577\" target=\"_blank\" rel=\"noopener\">Stanford study\u003c/a> is the first to replicate this in humans.\u003c/p>\n\u003cp>They believe this brain marker is a much more robust, dependable predictor of who will relapse, as opposed to users reporting cravings or environmental triggers. The study showed that users themselves cannot predict their own likelihood of relapse.\u003c/p>\n\u003cp>So even though Dee Dee could taste drugs in the back of her throat when thinking about pictures of dope, in the end, that may have no bearing on her risk of relapse. In MacNiven’s first round of tests, what former drug users said they wanted had no relation to what their brains said they wanted, MacNiven says. Self-reports did not predict who ended up relapsing and who didn’t. Only the brain activity did.\u003c/p>\n\u003cp>“We actually think this is interesting and might be a factor related to addiction, meaning that you might not have the ability to really know what you want,” MacNiven says.\u003c/p>\n\u003cp>To be sure of this conclusion, researchers have to test more people. They did the first round of scans on veterans — almost all men. Historically, this is true of a lot of addiction research. MacNiven is now actively recruiting and testing women to make sure her results hold up.\u003c/p>\n\u003cp>“This confirmation is vital, as women with stimulant use disorders may have more intense craving after drug cessation,” wrote Jay Nierenberg, a psychiatry professor at NYU School of Medicine, in \u003ca href=\"https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2719570\" target=\"_blank\" rel=\"noopener\">a paper\u003c/a> reviewing the Stanford results among vets. “And poorer clinical outcomes among women with stimulant use disorders have been reported in multiple studies.”\u003c/p>\n\u003cfigure id=\"attachment_11728951\" class=\"wp-caption aligncenter\" style=\"max-width: 800px\">\u003cimg class=\"size-medium wp-image-11728951\" src=\"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2019/02/Needle-and-spoon-800x600.jpg\" alt=\"\" width=\"800\" height=\"600\">\u003cfigcaption class=\"wp-caption-text\">What former users said they wanted had no bearing on whether they went on to relapse. \u003ccite>(April Dembosky/KQED)\u003c/cite>\u003c/figcaption>\u003c/figure>\n\u003cp>\u003cstrong>Implications for Treatment\u003c/strong>\u003c/p>\n\u003cp>If the findings do hold up in a larger, more diverse population, the implications could be powerful. Treatment providers could tailor care more specifically and target more precisely who should get what kind of treatment and for how long.\u003c/p>\n\u003cp>“Identifying those at greatest risk and providing treatment that specifically targets modifiable components of that risk would undoubtedly change the landscape of substance abuse treatment, likely attracting more people who need it and perhaps reducing burnout among those who provide it,” Nierenberg writes.\u003c/p>\n\u003cp>But it also means the only way to know who’s at highest risk for relapse requires giving everyone an MRI.\u003c/p>\n\u003cp>“I would say, is that so bad?” MacNiven asks. “Doing a $400 MRI scan, if that actually keeps people from relapsing, then I would say that it’s worth it.”\u003c/p>\n\u003cp>But of course getting access to this kind of diagnostic care is much more complicated than that. Not everyone who needs help with relapse lives near Stanford, or any MRI lab, and the details of this experiment are complex and difficult to emulate in other clinical settings. Plus, the scans take six hours for each test subject — not everyone can tolerate being enclosed in a tight, noisy machine for that long.\u003c/p>\n\u003cp>\"These results help to advance the field, although use in clinical practice is unlikely, at least for the time being,\" says Dr. Phillip Coffin, director of substance use research at the San Francisco Department of Public Health.\u003c/p>\n\u003cp>Then there is the question of effective treatments. There are no Food and Drug Administration-approved \u003ca href=\"https://www.kqed.org/news/11728012/lack-of-medication-treatments-for-meth-frustrates-doctors\" target=\"_blank\" rel=\"noopener\">medications for stimulant addiction\u003c/a> the way there are for opioids.\u003c/p>\n\u003cp>MacNiven and her team are brainstorming other options from their research — things like magnetic stimulation of the scalp to interfere with the brain’s addiction activity. Or neurofeedback, where users train their own brains not to light up at the sight of drugs.\u003c/p>\n\u003cp>“The idea that there could be anything that is an option for people, that is not the conventional standard stuff, is really exciting to people,” MacNiven says, “even if it’s something like brain zapping.”\u003c/p>\n\u003cp>That would be a relief to folks like Dee Dee. She’s been in treatment for four months so far at the \u003ca href=\"https://www.theepiphanycenter.org/\" target=\"_blank\" rel=\"noopener\">Epiphany Center\u003c/a>, a residential program for women in San Francisco. She admits her initial interest in participating in the study was for the free lunch and the Amazon gift card. But that changed the more she understood the research goals.\u003c/p>\n\u003cp>\u003c/p>\u003c/div>","attributes":{"named":{},"numeric":[]}},{"type":"component","content":"","name":"ad","attributes":{"named":{"label":"floatright"},"numeric":["floatright"]}},{"type":"contentString","content":"\u003cdiv class=\"post-body\">\u003cp>\u003c/p>\n\u003cp>“Anything that I can use to help people understand why we do the things we do, or maybe help someone to say no to drugs?” she says, “I'm all for it.”\u003c/p>\n\n\u003c/div>\u003c/p>","attributes":{"named":{},"numeric":[]}}],"link":"/news/11728856/stanford-researchers-using-mri-scans-to-predict-meth-and-cocaine-relapse","authors":["3205"],"programs":["news_72"],"categories":["news_457","news_8","news_356"],"tags":["news_21434","news_25076","news_24982"],"featImg":"news_11728942","label":"news_72","isLoading":false,"hasAllInfo":true}},"programsReducer":{"possible":{"id":"possible","title":"Possible","info":"Possible is hosted by entrepreneur Reid Hoffman and writer Aria Finger. Together in Possible, Hoffman and Finger lead enlightening discussions about building a brighter collective future. The show features interviews with visionary guests like Trevor Noah, Sam Altman and Janette Sadik-Khan. Possible paints an optimistic portrait of the world we can create through science, policy, business, art and our shared humanity. It asks: What if everything goes right for once? How can we get there? Each episode also includes a short fiction story generated by advanced AI GPT-4, serving as a thought-provoking springboard to speculate how humanity could leverage technology for good.","airtime":"SUN 2pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Possible-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.possible.fm/","meta":{"site":"news","source":"Possible"},"link":"/radio/program/possible","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/possible/id1677184070","spotify":"https://open.spotify.com/show/730YpdUSNlMyPQwNnyjp4k"}},"1a":{"id":"1a","title":"1A","info":"1A is home to the national conversation. 1A brings on great guests and frames the best debate in ways that make you think, share and engage.","airtime":"MON-THU 11pm-12am","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/1a.jpg","officialWebsiteLink":"https://the1a.org/","meta":{"site":"news","source":"npr"},"link":"/radio/program/1a","subscribe":{"npr":"https://rpb3r.app.goo.gl/RBrW","apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=1188724250&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/1A-p947376/","rss":"https://feeds.npr.org/510316/podcast.xml"}},"all-things-considered":{"id":"all-things-considered","title":"All Things Considered","info":"Every weekday, \u003cem>All Things Considered\u003c/em> hosts Robert Siegel, Audie Cornish, Ari Shapiro, and Kelly McEvers present the program's trademark mix of news, interviews, commentaries, reviews, and offbeat features. Michel Martin hosts on the weekends.","airtime":"MON-FRI 1pm-2pm, 4:30pm-6:30pm\u003cbr />SAT-SUN 5pm-6pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/All-Things-Considered-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.npr.org/programs/all-things-considered/","meta":{"site":"news","source":"npr"},"link":"/radio/program/all-things-considered"},"american-suburb-podcast":{"id":"american-suburb-podcast","title":"American Suburb: The Podcast","tagline":"The flip side of gentrification, told through one town","info":"Gentrification is changing cities across America, forcing people from neighborhoods they have long called home. Call them the displaced. Now those priced out of the Bay Area are looking for a better life in an unlikely place. American Suburb follows this migration to one California town along the Delta, 45 miles from San Francisco. But is this once sleepy suburb ready for them?","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/American-Suburb-Podcast-Tile-703x703-1.jpg","officialWebsiteLink":"/news/series/american-suburb-podcast","meta":{"site":"news","source":"kqed","order":"13"},"link":"/news/series/american-suburb-podcast/","subscribe":{"npr":"https://rpb3r.app.goo.gl/RBrW","apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?mt=2&id=1287748328","tuneIn":"https://tunein.com/radio/American-Suburb-p1086805/","rss":"https://ww2.kqed.org/news/series/american-suburb-podcast/feed/podcast","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkMzMDExODgxNjA5"}},"baycurious":{"id":"baycurious","title":"Bay Curious","tagline":"Exploring the Bay Area, one question at a time","info":"KQED’s new podcast, Bay Curious, gets to the bottom of the mysteries — both profound and peculiar — that give the Bay Area its unique identity. And we’ll do it with your help! You ask the questions. You decide what Bay Curious investigates. And you join us on the journey to find the answers.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Bay-Curious-Podcast-Tile-703x703-1.jpg","imageAlt":"\"KQED Bay Curious","officialWebsiteLink":"/news/series/baycurious","meta":{"site":"news","source":"kqed","order":"4"},"link":"/podcasts/baycurious","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/bay-curious/id1172473406","npr":"https://www.npr.org/podcasts/500557090/bay-curious","rss":"https://ww2.kqed.org/news/category/bay-curious-podcast/feed/podcast","google":"https://podcasts.google.com/feed/aHR0cHM6Ly93dzIua3FlZC5vcmcvbmV3cy9jYXRlZ29yeS9iYXktY3VyaW91cy1wb2RjYXN0L2ZlZWQvcG9kY2FzdA","stitcher":"https://www.stitcher.com/podcast/kqed/bay-curious","spotify":"https://open.spotify.com/show/6O76IdmhixfijmhTZLIJ8k"}},"bbc-world-service":{"id":"bbc-world-service","title":"BBC World Service","info":"The day's top stories from BBC News compiled twice daily in the week, once at weekends.","airtime":"MON-FRI 9pm-10pm, TUE-FRI 1am-2am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/BBC-World-Service-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.bbc.co.uk/sounds/play/live:bbc_world_service","meta":{"site":"news","source":"BBC World Service"},"link":"/radio/program/bbc-world-service","subscribe":{"apple":"https://itunes.apple.com/us/podcast/global-news-podcast/id135067274?mt=2","tuneIn":"https://tunein.com/radio/BBC-World-Service-p455581/","rss":"https://podcasts.files.bbci.co.uk/p02nq0gn.rss"}},"code-switch-life-kit":{"id":"code-switch-life-kit","title":"Code Switch / Life Kit","info":"\u003cem>Code Switch\u003c/em>, which listeners will hear in the first part of the hour, has fearless and much-needed conversations about race. Hosted by journalists of color, the show tackles the subject of race head-on, exploring how it impacts every part of society — from politics and pop culture to history, sports and more.\u003cbr />\u003cbr />\u003cem>Life Kit\u003c/em>, which will be in the second part of the hour, guides you through spaces and feelings no one prepares you for — from finances to mental health, from workplace microaggressions to imposter syndrome, from relationships to parenting. The show features experts with real world experience and shares their knowledge. Because everyone needs a little help being human.\u003cbr />\u003cbr />\u003ca href=\"https://www.npr.org/podcasts/510312/codeswitch\">\u003cem>Code Switch\u003c/em> offical site and podcast\u003c/a>\u003cbr />\u003ca href=\"https://www.npr.org/lifekit\">\u003cem>Life Kit\u003c/em> offical site and podcast\u003c/a>\u003cbr />","airtime":"SUN 9pm-10pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Code-Switch-Life-Kit-Podcast-Tile-360x360-1.jpg","meta":{"site":"radio","source":"npr"},"link":"/radio/program/code-switch-life-kit","subscribe":{"apple":"https://podcasts.apple.com/podcast/1112190608?mt=2&at=11l79Y&ct=nprdirectory","google":"https://podcasts.google.com/feed/aHR0cHM6Ly93d3cubnByLm9yZy9yc3MvcG9kY2FzdC5waHA_aWQ9NTEwMzEy","spotify":"https://open.spotify.com/show/3bExJ9JQpkwNhoHvaIIuyV","rss":"https://feeds.npr.org/510312/podcast.xml"}},"commonwealth-club":{"id":"commonwealth-club","title":"Commonwealth Club of California Podcast","info":"The Commonwealth Club of California is the nation's oldest and largest public affairs forum. As a non-partisan forum, The Club brings to the public airwaves diverse viewpoints on important topics. The Club's weekly radio broadcast - the oldest in the U.S., dating back to 1924 - is carried across the nation on public radio stations and is now podcasting. Our website archive features audio of our recent programs, as well as selected speeches from our long and distinguished history. This podcast feed is usually updated twice a week and is always un-edited.","airtime":"THU 10pm, FRI 1am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Commonwealth-Club-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.commonwealthclub.org/podcasts","meta":{"site":"news","source":"Commonwealth Club of California"},"link":"/radio/program/commonwealth-club","subscribe":{"apple":"https://itunes.apple.com/us/podcast/commonwealth-club-of-california-podcast/id976334034?mt=2","google":"https://podcasts.google.com/feed/aHR0cDovL3d3dy5jb21tb253ZWFsdGhjbHViLm9yZy9hdWRpby9wb2RjYXN0L3dlZWtseS54bWw","tuneIn":"https://tunein.com/radio/Commonwealth-Club-of-California-p1060/"}},"considerthis":{"id":"considerthis","title":"Consider This","tagline":"Make sense of the day","info":"Make sense of the day. Every weekday afternoon, Consider This helps you consider the major stories of the day in less than 15 minutes, featuring the reporting and storytelling resources of NPR. Plus, KQED’s Bianca Taylor brings you the local KQED news you need to know.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Consider-This-Podcast-Tile-703x703-1.jpg","imageAlt":"Consider This from NPR and KQED","officialWebsiteLink":"/podcasts/considerthis","meta":{"site":"news","source":"kqed","order":"7"},"link":"/podcasts/considerthis","subscribe":{"apple":"https://podcasts.apple.com/podcast/id1503226625?mt=2&at=11l79Y&ct=nprdirectory","npr":"https://rpb3r.app.goo.gl/coronavirusdaily","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5ucHIub3JnLzUxMDM1NS9wb2RjYXN0LnhtbA","spotify":"https://open.spotify.com/show/3Z6JdCS2d0eFEpXHKI6WqH"}},"forum":{"id":"forum","title":"Forum","tagline":"The conversation starts here","info":"KQED’s live call-in program discussing local, state, national and international issues, as well as in-depth interviews.","airtime":"MON-FRI 9am-11am, 10pm-11pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Forum-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED Forum with Mina Kim and Alexis Madrigal","officialWebsiteLink":"/forum","meta":{"site":"news","source":"kqed","order":"8"},"link":"/forum","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/kqeds-forum/id73329719","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM5NTU3MzgxNjMz","npr":"https://www.npr.org/podcasts/432307980/forum","stitcher":"https://www.stitcher.com/podcast/kqedfm-kqeds-forum-podcast","rss":"https://feeds.megaphone.fm/KQINC9557381633"}},"freakonomics-radio":{"id":"freakonomics-radio","title":"Freakonomics Radio","info":"Freakonomics Radio is a one-hour award-winning podcast and public-radio project hosted by Stephen Dubner, with co-author Steve Levitt as a regular guest. It is produced in partnership with WNYC.","imageSrc":"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2018/05/freakonomicsRadio.png","officialWebsiteLink":"http://freakonomics.com/","airtime":"SUN 1am-2am, SAT 3pm-4pm","meta":{"site":"radio","source":"WNYC"},"link":"/radio/program/freakonomics-radio","subscribe":{"npr":"https://rpb3r.app.goo.gl/4s8b","apple":"https://itunes.apple.com/us/podcast/freakonomics-radio/id354668519","tuneIn":"https://tunein.com/podcasts/WNYC-Podcasts/Freakonomics-Radio-p272293/","rss":"https://feeds.feedburner.com/freakonomicsradio"}},"fresh-air":{"id":"fresh-air","title":"Fresh Air","info":"Hosted by Terry Gross, \u003cem>Fresh Air from WHYY\u003c/em> is the Peabody Award-winning weekday magazine of contemporary arts and issues. One of public radio's most popular programs, Fresh Air features intimate conversations with today's biggest luminaries.","airtime":"MON-FRI 7pm-8pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Fresh-Air-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.npr.org/programs/fresh-air/","meta":{"site":"radio","source":"npr"},"link":"/radio/program/fresh-air","subscribe":{"npr":"https://rpb3r.app.goo.gl/4s8b","apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=214089682&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/Fresh-Air-p17/","rss":"https://feeds.npr.org/381444908/podcast.xml"}},"here-and-now":{"id":"here-and-now","title":"Here & Now","info":"A live production of NPR and WBUR Boston, in collaboration with stations across the country, Here & Now reflects the fluid world of news as it's happening in the middle of the day, with timely, in-depth news, interviews and conversation. Hosted by Robin Young, Jeremy Hobson and Tonya Mosley.","airtime":"MON-THU 11am-12pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Here-And-Now-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"http://www.wbur.org/hereandnow","meta":{"site":"news","source":"npr"},"link":"/radio/program/here-and-now","subsdcribe":{"apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?mt=2&id=426698661","tuneIn":"https://tunein.com/radio/Here--Now-p211/","rss":"https://feeds.npr.org/510051/podcast.xml"}},"how-i-built-this":{"id":"how-i-built-this","title":"How I Built This with Guy Raz","info":"Guy Raz dives into the stories behind some of the world's best known companies. How I Built This weaves a narrative journey about innovators, entrepreneurs and idealists—and the movements they built.","imageSrc":"https://ww2.kqed.org/news/wp-content/uploads/sites/10/2018/05/howIBuiltThis.png","officialWebsiteLink":"https://www.npr.org/podcasts/510313/how-i-built-this","airtime":"SUN 7:30pm-8pm","meta":{"site":"news","source":"npr"},"link":"/radio/program/how-i-built-this","subscribe":{"npr":"https://rpb3r.app.goo.gl/3zxy","apple":"https://itunes.apple.com/us/podcast/how-i-built-this-with-guy-raz/id1150510297?mt=2","tuneIn":"https://tunein.com/podcasts/Arts--Culture-Podcasts/How-I-Built-This-p910896/","rss":"https://feeds.npr.org/510313/podcast.xml"}},"inside-europe":{"id":"inside-europe","title":"Inside Europe","info":"Inside Europe, a one-hour weekly news magazine hosted by Helen Seeney and Keith Walker, explores the topical issues shaping the continent. No other part of the globe has experienced such dynamic political and social change in recent years.","airtime":"SAT 3am-4am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Inside-Europe-Podcast-Tile-300x300-1.jpg","meta":{"site":"news","source":"Deutsche Welle"},"link":"/radio/program/inside-europe","subscribe":{"apple":"https://itunes.apple.com/us/podcast/inside-europe/id80106806?mt=2","tuneIn":"https://tunein.com/radio/Inside-Europe-p731/","rss":"https://partner.dw.com/xml/podcast_inside-europe"}},"latino-usa":{"id":"latino-usa","title":"Latino USA","airtime":"MON 1am-2am, SUN 6pm-7pm","info":"Latino USA, the radio journal of news and culture, is the only national, English-language radio program produced from a Latino perspective.","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/latinoUsa.jpg","officialWebsiteLink":"http://latinousa.org/","meta":{"site":"news","source":"npr"},"link":"/radio/program/latino-usa","subscribe":{"npr":"https://rpb3r.app.goo.gl/xtTd","apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=79681317&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/Latino-USA-p621/","rss":"https://feeds.npr.org/510016/podcast.xml"}},"live-from-here-highlights":{"id":"live-from-here-highlights","title":"Live from Here Highlights","info":"Chris Thile steps to the mic as the host of Live from Here (formerly A Prairie Home Companion), a live public radio variety show. Download Chris’s Song of the Week plus other highlights from the broadcast. Produced by American Public Media.","airtime":"SAT 6pm-8pm, SUN 11am-1pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Live-From-Here-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.livefromhere.org/","meta":{"site":"arts","source":"american public media"},"link":"/radio/program/live-from-here-highlights","subscribe":{"apple":"https://itunes.apple.com/us/podcast/id1167173941","tuneIn":"https://tunein.com/radio/Live-from-Here-Highlights-p921744/","rss":"https://feeds.publicradio.org/public_feeds/a-prairie-home-companion-highlights/rss/rss"}},"marketplace":{"id":"marketplace","title":"Marketplace","info":"Our flagship program, helmed by Kai Ryssdal, examines what the day in money delivered, through stories, conversations, newsworthy numbers and more. Updated Monday through Friday at about 3:30 p.m. PT.","airtime":"MON-FRI 4pm-4:30pm, MON-WED 6:30pm-7pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Marketplace-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.marketplace.org/","meta":{"site":"news","source":"American Public Media"},"link":"/radio/program/marketplace","subscribe":{"apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=201853034&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/APM-Marketplace-p88/","rss":"https://feeds.publicradio.org/public_feeds/marketplace-pm/rss/rss"}},"mindshift":{"id":"mindshift","title":"MindShift","tagline":"A podcast about the future of learning and how we raise our kids","info":"The MindShift podcast explores the innovations in education that are shaping how kids learn. Hosts Ki Sung and Katrina Schwartz introduce listeners to educators, researchers, parents and students who are developing effective ways to improve how kids learn. We cover topics like how fed-up administrators are developing surprising tactics to deal with classroom disruptions; how listening to podcasts are helping kids develop reading skills; the consequences of overparenting; and why interdisciplinary learning can engage students on all ends of the traditional achievement spectrum. This podcast is part of the MindShift education site, a division of KQED News. KQED is an NPR/PBS member station based in San Francisco. You can also visit the MindShift website for episodes and supplemental blog posts or tweet us \u003ca href=\"https://twitter.com/MindShiftKQED\">@MindShiftKQED\u003c/a> or visit us at \u003ca href=\"/mindshift\">MindShift.KQED.org\u003c/a>","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Mindshift-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED MindShift: How We Will Learn","officialWebsiteLink":"/mindshift/","meta":{"site":"news","source":"kqed","order":"2"},"link":"/podcasts/mindshift","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/mindshift-podcast/id1078765985","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM1NzY0NjAwNDI5","npr":"https://www.npr.org/podcasts/464615685/mind-shift-podcast","stitcher":"https://www.stitcher.com/podcast/kqed/stories-teachers-share","spotify":"https://open.spotify.com/show/0MxSpNYZKNprFLCl7eEtyx"}},"morning-edition":{"id":"morning-edition","title":"Morning Edition","info":"\u003cem>Morning Edition\u003c/em> takes listeners around the country and the world with multi-faceted stories and commentaries every weekday. Hosts Steve Inskeep, David Greene and Rachel Martin bring you the latest breaking news and features to prepare you for the day.","airtime":"MON-FRI 3am-9am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Morning-Edition-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.npr.org/programs/morning-edition/","meta":{"site":"news","source":"npr"},"link":"/radio/program/morning-edition"},"onourwatch":{"id":"onourwatch","title":"On Our Watch","tagline":"Police secrets, unsealed","info":"For decades, the process for how police police themselves has been inconsistent – if not opaque. In some states, like California, these proceedings were completely hidden. After a new police transparency law unsealed scores of internal affairs files, our reporters set out to examine these cases and the shadow world of police discipline. On Our Watch brings listeners into the rooms where officers are questioned and witnesses are interrogated to find out who this system is really protecting. Is it the officers, or the public they've sworn to serve?","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/On-Our-Watch-Podcast-Tile-703x703-1.jpg","imageAlt":"On Our Watch from NPR and KQED","officialWebsiteLink":"/podcasts/onourwatch","meta":{"site":"news","source":"kqed","order":"1"},"link":"/podcasts/onourwatch","subscribe":{"apple":"https://podcasts.apple.com/podcast/id1567098962","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5ucHIub3JnLzUxMDM2MC9wb2RjYXN0LnhtbD9zYz1nb29nbGVwb2RjYXN0cw","npr":"https://rpb3r.app.goo.gl/onourwatch","spotify":"https://open.spotify.com/show/0OLWoyizopu6tY1XiuX70x","tuneIn":"https://tunein.com/radio/On-Our-Watch-p1436229/","stitcher":"https://www.stitcher.com/show/on-our-watch","rss":"https://feeds.npr.org/510360/podcast.xml"}},"on-the-media":{"id":"on-the-media","title":"On The Media","info":"Our weekly podcast explores how the media 'sausage' is made, casts an incisive eye on fluctuations in the marketplace of ideas, and examines threats to the freedom of information and expression in America and abroad. For one hour a week, the show tries to lift the veil from the process of \"making media,\" especially news media, because it's through that lens that we see the world and the world sees us","airtime":"SUN 2pm-3pm, MON 12am-1am","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/onTheMedia.png","officialWebsiteLink":"https://www.wnycstudios.org/shows/otm","meta":{"site":"news","source":"wnyc"},"link":"/radio/program/on-the-media","subscribe":{"apple":"https://itunes.apple.com/us/podcast/on-the-media/id73330715?mt=2","tuneIn":"https://tunein.com/radio/On-the-Media-p69/","rss":"http://feeds.wnyc.org/onthemedia"}},"our-body-politic":{"id":"our-body-politic","title":"Our Body Politic","info":"Presented by KQED, KCRW and KPCC, and created and hosted by award-winning journalist Farai Chideya, Our Body Politic is unapologetically centered on reporting on not just how women of color experience the major political events of today, but how they’re impacting those very issues.","airtime":"SAT 6pm-7pm, SUN 1am-2am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Our-Body-Politic-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://our-body-politic.simplecast.com/","meta":{"site":"news","source":"kcrw"},"link":"/radio/program/our-body-politic","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/our-body-politic/id1533069868","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5zaW1wbGVjYXN0LmNvbS9feGFQaHMxcw","spotify":"https://open.spotify.com/show/4ApAiLT1kV153TttWAmqmc","rss":"https://feeds.simplecast.com/_xaPhs1s","tuneIn":"https://tunein.com/podcasts/News--Politics-Podcasts/Our-Body-Politic-p1369211/"}},"pbs-newshour":{"id":"pbs-newshour","title":"PBS NewsHour","info":"Analysis, background reports and updates from the PBS NewsHour putting today's news in context.","airtime":"MON-FRI 3pm-4pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/PBS-News-Hour-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.pbs.org/newshour/","meta":{"site":"news","source":"pbs"},"link":"/radio/program/pbs-newshour","subscribe":{"apple":"https://itunes.apple.com/us/podcast/pbs-newshour-full-show/id394432287?mt=2","tuneIn":"https://tunein.com/radio/PBS-NewsHour---Full-Show-p425698/","rss":"https://www.pbs.org/newshour/feeds/rss/podcasts/show"}},"perspectives":{"id":"perspectives","title":"Perspectives","tagline":"KQED's series of of daily listener commentaries since 1991","info":"KQED's series of of daily listener commentaries since 1991.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Perspectives-Podcast-Tile-703x703-1.jpg","officialWebsiteLink":"/perspectives/","meta":{"site":"radio","source":"kqed","order":"15"},"link":"/perspectives","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/id73801135","npr":"https://www.npr.org/podcasts/432309616/perspectives","rss":"https://ww2.kqed.org/perspectives/category/perspectives/feed/","google":"https://podcasts.google.com/feed/aHR0cHM6Ly93dzIua3FlZC5vcmcvcGVyc3BlY3RpdmVzL2NhdGVnb3J5L3BlcnNwZWN0aXZlcy9mZWVkLw"}},"planet-money":{"id":"planet-money","title":"Planet Money","info":"The economy explained. Imagine you could call up a friend and say, Meet me at the bar and tell me what's going on with the economy. Now imagine that's actually a fun evening.","airtime":"SUN 3pm-4pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/planetmoney.jpg","officialWebsiteLink":"https://www.npr.org/sections/money/","meta":{"site":"news","source":"npr"},"link":"/radio/program/planet-money","subscribe":{"npr":"https://rpb3r.app.goo.gl/M4f5","apple":"https://itunes.apple.com/us/podcast/planet-money/id290783428?mt=2","tuneIn":"https://tunein.com/podcasts/Business--Economics-Podcasts/Planet-Money-p164680/","rss":"https://feeds.npr.org/510289/podcast.xml"}},"politicalbreakdown":{"id":"politicalbreakdown","title":"Political Breakdown","tagline":"Politics from a personal perspective","info":"Political Breakdown is a new series that explores the political intersection of California and the nation. Each week hosts Scott Shafer and Marisa Lagos are joined with a new special guest to unpack politics -- with personality — and offer an insider’s glimpse at how politics happens.","airtime":"THU 6:30pm-7pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Political-Breakdown-2024-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED Political Breakdown","officialWebsiteLink":"/podcasts/politicalbreakdown","meta":{"site":"radio","source":"kqed","order":"11"},"link":"/podcasts/politicalbreakdown","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/political-breakdown/id1327641087","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM5Nzk2MzI2MTEx","npr":"https://www.npr.org/podcasts/572155894/political-breakdown","stitcher":"https://www.stitcher.com/podcast/kqed/political-breakdown","spotify":"https://open.spotify.com/show/07RVyIjIdk2WDuVehvBMoN","rss":"https://ww2.kqed.org/news/tag/political-breakdown/feed/podcast"}},"pri-the-world":{"id":"pri-the-world","title":"PRI's The World: Latest Edition","info":"Each weekday, host Marco Werman and his team of producers bring you the world's most interesting stories in an hour of radio that reminds us just how small our planet really is.","airtime":"MON-FRI 2pm-3pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-World-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.pri.org/programs/the-world","meta":{"site":"news","source":"PRI"},"link":"/radio/program/pri-the-world","subscribe":{"apple":"https://itunes.apple.com/us/podcast/pris-the-world-latest-edition/id278196007?mt=2","tuneIn":"https://tunein.com/podcasts/News--Politics-Podcasts/PRIs-The-World-p24/","rss":"http://feeds.feedburner.com/pri/theworld"}},"radiolab":{"id":"radiolab","title":"Radiolab","info":"A two-time Peabody Award-winner, Radiolab is an investigation told through sounds and stories, and centered around one big idea. In the Radiolab world, information sounds like music and science and culture collide. Hosted by Jad Abumrad and Robert Krulwich, the show is designed for listeners who demand skepticism, but appreciate wonder. WNYC Studios is the producer of other leading podcasts including Freakonomics Radio, Death, Sex & Money, On the Media and many more.","airtime":"SUN 12am-1am, SAT 2pm-3pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/radiolab1400.png","officialWebsiteLink":"https://www.wnycstudios.org/shows/radiolab/","meta":{"site":"science","source":"WNYC"},"link":"/radio/program/radiolab","subscribe":{"apple":"https://itunes.apple.com/us/podcast/radiolab/id152249110?mt=2","tuneIn":"https://tunein.com/radio/RadioLab-p68032/","rss":"https://feeds.wnyc.org/radiolab"}},"reveal":{"id":"reveal","title":"Reveal","info":"Created by The Center for Investigative Reporting and PRX, Reveal is public radios first one-hour weekly radio show and podcast dedicated to investigative reporting. Credible, fact based and without a partisan agenda, Reveal combines the power and artistry of driveway moment storytelling with data-rich reporting on critically important issues. The result is stories that inform and inspire, arming our listeners with information to right injustices, hold the powerful accountable and improve lives.Reveal is hosted by Al Letson and showcases the award-winning work of CIR and newsrooms large and small across the nation. In a radio and podcast market crowded with choices, Reveal focuses on important and often surprising stories that illuminate the world for our listeners.","airtime":"SAT 4pm-5pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/reveal300px.png","officialWebsiteLink":"https://www.revealnews.org/episodes/","meta":{"site":"news","source":"npr"},"link":"/radio/program/reveal","subscribe":{"apple":"https://itunes.apple.com/us/podcast/reveal/id886009669","tuneIn":"https://tunein.com/radio/Reveal-p679597/","rss":"http://feeds.revealradio.org/revealpodcast"}},"says-you":{"id":"says-you","title":"Says You!","info":"Public radio's game show of bluff and bluster, words and whimsy. The warmest, wittiest cocktail party - it's spirited and civil, brainy and boisterous, peppered with musical interludes. Fast paced and playful, it's the most fun you can have with language without getting your mouth washed out with soap. Our motto: It's not important to know the answers, it's important to like the answers!","airtime":"SUN 4pm-5pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Says-You-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"http://www.saysyouradio.com/","meta":{"site":"comedy","source":"Pipit and Finch"},"link":"/radio/program/says-you","subscribe":{"apple":"https://itunes.apple.com/us/podcast/says-you!/id1050199826","tuneIn":"https://tunein.com/radio/Says-You-p480/","rss":"https://saysyou.libsyn.com/rss"}},"science-friday":{"id":"science-friday","title":"Science Friday","info":"Science Friday is a weekly science talk show, broadcast live over public radio stations nationwide. Each week, the show focuses on science topics that are in the news and tries to bring an educated, balanced discussion to bear on the scientific issues at hand. Panels of expert guests join host Ira Flatow, a veteran science journalist, to discuss science and to take questions from listeners during the call-in portion of the program.","airtime":"FRI 11am-1pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Science-Friday-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.wnycstudios.org/shows/science-friday","meta":{"site":"news","source":"npr"},"link":"/radio/program/science-friday","subscribe":{"apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=73329284&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/Science-Friday-p394/","rss":"http://feeds.wnyc.org/science-friday"}},"science-podcast":{"id":"science-podcast","title":"KQED Science News","tagline":"From the lab, to your ears","info":"KQED Science explores science and environment news, trends, and events from the Bay Area and beyond.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Science-News-Podcast-Tile-703x703-1.jpg","officialWebsiteLink":"https://ww2.kqed.org/science/category/science-podcast/","meta":{"site":"science","source":"kqed","order":"17"},"link":"/science/category/science-podcast","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/kqed-science-news/id214663465","google":"https://podcasts.google.com/feed/aHR0cDovL2Jsb2dzLmtxZWQub3JnL3NjaWVuY2UvZmVlZC8","stitcher":"https://www.stitcher.com/podcast/kqed-science-news","rss":"https://ww2.kqed.org/science/category/science-podcast/feed/podcast"}},"selected-shorts":{"id":"selected-shorts","title":"Selected Shorts","info":"Spellbinding short stories by established and emerging writers take on a new life when they are performed by stars of the stage and screen.","airtime":"SAT 8pm-9pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Selected-Shorts-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.pri.org/programs/selected-shorts","meta":{"site":"arts","source":"pri"},"link":"/radio/program/selected-shorts","subscribe":{"apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=253191824&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/Selected-Shorts-p31792/","rss":"https://feeds.megaphone.fm/selectedshorts"}},"snap-judgment":{"id":"snap-judgment","title":"Snap Judgment","info":"Snap Judgment (Storytelling, with a BEAT) mixes real stories with killer beats to produce cinematic, dramatic, kick-ass radio. Snap’s raw, musical brand of storytelling dares listeners to see the world through the eyes of another. WNYC studios is the producer of leading podcasts including Radiolab, Freakonomics Radio, Note To Self, Here’s The Thing With Alec Baldwin, and more.","airtime":"SAT 1pm-2pm, 9pm-10pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/snapJudgement.jpg","officialWebsiteLink":"https://snapjudgment.org","meta":{"site":"arts","source":"WNYC"},"link":"/radio/program/snap-judgment","subscribe":{"apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=283657561&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/Snap-Judgment-p243817/","rss":"https://feeds.feedburner.com/snapjudgment-wnyc"}},"soldout":{"id":"soldout","title":"SOLD OUT: Rethinking Housing in America","tagline":"A new future for housing","info":"Sold Out: Rethinking Housing in America","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Sold-Out-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED Sold Out: Rethinking Housing in America","officialWebsiteLink":"/podcasts/soldout","meta":{"site":"news","source":"kqed","order":3},"link":"/podcasts/soldout","subscribe":{"npr":"https://www.npr.org/podcasts/911586047/s-o-l-d-o-u-t-a-new-future-for-housing","apple":"https://podcasts.apple.com/us/podcast/introducing-sold-out-rethinking-housing-in-america/id1531354937","rss":"https://feeds.megaphone.fm/soldout","spotify":"https://open.spotify.com/show/38dTBSk2ISFoPiyYNoKn1X","stitcher":"https://www.stitcher.com/podcast/kqed/sold-out-rethinking-housing-in-america","tunein":"https://tunein.com/radio/SOLD-OUT-Rethinking-Housing-in-America-p1365871/","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vc29sZG91dA"}},"ted-radio-hour":{"id":"ted-radio-hour","title":"TED Radio Hour","info":"The TED Radio Hour is a journey through fascinating ideas, astonishing inventions, fresh approaches to old problems, and new ways to think and create.","airtime":"SUN 3pm-4pm, SAT 10pm-11pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/tedRadioHour.jpg","officialWebsiteLink":"https://www.npr.org/programs/ted-radio-hour/?showDate=2018-06-22","meta":{"site":"news","source":"npr"},"link":"/radio/program/ted-radio-hour","subscribe":{"npr":"https://rpb3r.app.goo.gl/8vsS","apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=523121474&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/TED-Radio-Hour-p418021/","rss":"https://feeds.npr.org/510298/podcast.xml"}},"tech-nation":{"id":"tech-nation","title":"Tech Nation Radio Podcast","info":"Tech Nation is a weekly public radio program, hosted by Dr. Moira Gunn. Founded in 1993, it has grown from a simple interview show to a multi-faceted production, featuring conversations with noted technology and science leaders, and a weekly science and technology-related commentary.","airtime":"FRI 10pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Tech-Nation-Radio-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"http://technation.podomatic.com/","meta":{"site":"science","source":"Tech Nation Media"},"link":"/radio/program/tech-nation","subscribe":{"rss":"https://technation.podomatic.com/rss2.xml"}},"thebay":{"id":"thebay","title":"The Bay","tagline":"Local news to keep you rooted","info":"Host Devin Katayama walks you through the biggest story of the day with reporters and newsmakers.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-Bay-Podcast-Tile-703x703-1.jpg","imageAlt":"\"KQED The Bay","officialWebsiteLink":"/podcasts/thebay","meta":{"site":"radio","source":"kqed","order":"6"},"link":"/podcasts/thebay","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/the-bay/id1350043452","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM4MjU5Nzg2MzI3","npr":"https://www.npr.org/podcasts/586725995/the-bay","stitcher":"https://www.stitcher.com/podcast/kqed/the-bay","spotify":"https://open.spotify.com/show/4BIKBKIujizLHlIlBNaAqQ","rss":"https://feeds.megaphone.fm/KQINC8259786327"}},"californiareport":{"id":"californiareport","title":"The California Report","tagline":"California, day by day","info":"KQED’s statewide radio news program providing daily coverage of issues, trends and public policy decisions.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-California-Report-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED The California Report","officialWebsiteLink":"/californiareport","meta":{"site":"news","source":"kqed","order":"9"},"link":"/californiareport","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/kqeds-the-california-report/id79681292","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM1MDAyODE4NTgz","npr":"https://www.npr.org/podcasts/432285393/the-california-report","stitcher":"https://www.stitcher.com/podcast/kqedfm-kqeds-the-california-report-podcast-8838","rss":"https://ww2.kqed.org/news/tag/tcram/feed/podcast"}},"californiareportmagazine":{"id":"californiareportmagazine","title":"The California Report Magazine","tagline":"Your state, your stories","info":"Every week, The California Report Magazine takes you on a road trip for the ears: to visit the places and meet the people who make California unique. The in-depth storytelling podcast from the California Report.","airtime":"FRI 4:30pm-5pm, 6:30pm-7pm, 11pm-11:30pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-California-Report-Magazine-Podcast-Tile-703x703-1.jpg","officialWebsiteLink":"/californiareportmagazine","meta":{"site":"news","source":"kqed","order":"10"},"link":"/californiareportmagazine","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/the-california-report-magazine/id1314750545","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM3NjkwNjk1OTAz","npr":"https://www.npr.org/podcasts/564733126/the-california-report-magazine","stitcher":"https://www.stitcher.com/podcast/kqed/the-california-report-magazine","rss":"https://ww2.kqed.org/news/tag/tcrmag/feed/podcast"}},"theleap":{"id":"theleap","title":"The Leap","tagline":"What if you closed your eyes, and jumped?","info":"Stories about people making dramatic, risky changes, told by award-winning public radio reporter Judy Campbell.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-Leap-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED The Leap","officialWebsiteLink":"/podcasts/theleap","meta":{"site":"news","source":"kqed","order":"14"},"link":"/podcasts/theleap","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/the-leap/id1046668171","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkM0NTcwODQ2MjY2","npr":"https://www.npr.org/podcasts/447248267/the-leap","stitcher":"https://www.stitcher.com/podcast/kqed/the-leap","spotify":"https://open.spotify.com/show/3sSlVHHzU0ytLwuGs1SD1U","rss":"https://ww2.kqed.org/news/programs/the-leap/feed/podcast"}},"masters-of-scale":{"id":"masters-of-scale","title":"Masters of Scale","info":"Masters of Scale is an original podcast in which LinkedIn co-founder and Greylock Partner Reid Hoffman sets out to describe and prove theories that explain how great entrepreneurs take their companies from zero to a gazillion in ingenious fashion.","airtime":"Every other Wednesday June 12 through October 16 at 8pm (repeats Thursdays at 2am)","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Masters-of-Scale-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://mastersofscale.com/","meta":{"site":"radio","source":"WaitWhat"},"link":"/radio/program/masters-of-scale","subscribe":{"apple":"http://mastersofscale.app.link/","rss":"https://rss.art19.com/masters-of-scale"}},"the-moth-radio-hour":{"id":"the-moth-radio-hour","title":"The Moth Radio Hour","info":"Since its launch in 1997, The Moth has presented thousands of true stories, told live and without notes, to standing-room-only crowds worldwide. Moth storytellers stand alone, under a spotlight, with only a microphone and a roomful of strangers. The storyteller and the audience embark on a high-wire act of shared experience which is both terrifying and exhilarating. Since 2008, The Moth podcast has featured many of our favorite stories told live on Moth stages around the country. For information on all of our programs and live events, visit themoth.org.","airtime":"SAT 8pm-9pm and SUN 11am-12pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/theMoth.jpg","officialWebsiteLink":"https://themoth.org/","meta":{"site":"arts","source":"prx"},"link":"/radio/program/the-moth-radio-hour","subscribe":{"apple":"https://itunes.apple.com/us/podcast/the-moth-podcast/id275699983?mt=2","tuneIn":"https://tunein.com/radio/The-Moth-p273888/","rss":"http://feeds.themoth.org/themothpodcast"}},"the-new-yorker-radio-hour":{"id":"the-new-yorker-radio-hour","title":"The New Yorker Radio Hour","info":"The New Yorker Radio Hour is a weekly program presented by the magazine's editor, David Remnick, and produced by WNYC Studios and The New Yorker. Each episode features a diverse mix of interviews, profiles, storytelling, and an occasional burst of humor inspired by the magazine, and shaped by its writers, artists, and editors. This isn't a radio version of a magazine, but something all its own, reflecting the rich possibilities of audio storytelling and conversation. Theme music for the show was composed and performed by Merrill Garbus of tUnE-YArDs.","airtime":"SAT 10am-11am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-New-Yorker-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.wnycstudios.org/shows/tnyradiohour","meta":{"site":"arts","source":"WNYC"},"link":"/radio/program/the-new-yorker-radio-hour","subscribe":{"apple":"https://itunes.apple.com/us/podcast/id1050430296","tuneIn":"https://tunein.com/podcasts/WNYC-Podcasts/New-Yorker-Radio-Hour-p803804/","rss":"https://feeds.feedburner.com/newyorkerradiohour"}},"the-takeaway":{"id":"the-takeaway","title":"The Takeaway","info":"The Takeaway is produced in partnership with its national audience. It delivers perspective and analysis to help us better understand the day’s news. Be a part of the American conversation on-air and online.","airtime":"MON-THU 12pm-1pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-Takeaway-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.wnycstudios.org/shows/takeaway","meta":{"site":"news","source":"WNYC"},"link":"/radio/program/the-takeaway","subscribe":{"apple":"https://itunes.apple.com/us/podcast/the-takeaway/id363143310?mt=2","tuneIn":"http://tunein.com/radio/The-Takeaway-p150731/","rss":"https://feeds.feedburner.com/takeawaypodcast"}},"this-american-life":{"id":"this-american-life","title":"This American Life","info":"This American Life is a weekly public radio show, heard by 2.2 million people on more than 500 stations. Another 2.5 million people download the weekly podcast. It is hosted by Ira Glass, produced in collaboration with Chicago Public Media, delivered to stations by PRX The Public Radio Exchange, and has won all of the major broadcasting awards.","airtime":"SAT 12pm-1pm, 7pm-8pm","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/thisAmericanLife.png","officialWebsiteLink":"https://www.thisamericanlife.org/","meta":{"site":"news","source":"wbez"},"link":"/radio/program/this-american-life","subscribe":{"apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=201671138&at=11l79Y&ct=nprdirectory","rss":"https://www.thisamericanlife.org/podcast/rss.xml"}},"truthbetold":{"id":"truthbetold","title":"Truth Be Told","tagline":"Advice by and for people of color","info":"We’re the friend you call after a long day, the one who gets it. Through wisdom from some of the greatest thinkers of our time, host Tonya Mosley explores what it means to grow and thrive as a Black person in America, while discovering new ways of being that serve as a portal to more love, more healing, and more joy.","airtime":"","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Truth-Be-Told-Podcast-Tile-360x360-1.jpg","imageAlt":"KQED Truth Be Told with Tonya Mosley","officialWebsiteLink":"https://www.kqed.ord/podcasts/truthbetold","meta":{"site":"news","source":"npr","order":"12"},"link":"/podcasts/truthbetold","subscribe":{"apple":"https://podcasts.apple.com/us/podcast/truth-be-told/id1462216572","google":"https://podcasts.google.com/feed/aHR0cHM6Ly93dzIua3FlZC5vcmcvbmV3cy9jYXRlZ29yeS90cnV0aC1iZS10b2xkLXBvZGNhc3QvZmVlZA","npr":"https://www.npr.org/podcasts/719210818/truth-be-told","stitcher":"https://www.stitcher.com/s?fid=398170&refid=stpr","spotify":"https://open.spotify.com/show/587DhwTBxke6uvfwDfaV5N"}},"wait-wait-dont-tell-me":{"id":"wait-wait-dont-tell-me","title":"Wait Wait... Don't Tell Me!","info":"Peter Sagal and Bill Kurtis host the weekly NPR News quiz show alongside some of the best and brightest news and entertainment personalities.","airtime":"SUN 10am-11am, SAT 11am-12pm, SAT 6pm-7pm","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Wait-Wait-Podcast-Tile-300x300-1.jpg","officialWebsiteLink":"https://www.npr.org/programs/wait-wait-dont-tell-me/","meta":{"site":"news","source":"npr"},"link":"/radio/program/wait-wait-dont-tell-me","subscribe":{"npr":"https://rpb3r.app.goo.gl/Xogv","apple":"https://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?s=143441&mt=2&id=121493804&at=11l79Y&ct=nprdirectory","tuneIn":"https://tunein.com/radio/Wait-Wait-Dont-Tell-Me-p46/","rss":"https://feeds.npr.org/344098539/podcast.xml"}},"washington-week":{"id":"washington-week","title":"Washington Week","info":"For 50 years, Washington Week has been the most intelligent and up to date conversation about the most important news stories of the week. Washington Week is the longest-running news and public affairs program on PBS and features journalists -- not pundits -- lending insight and perspective to the week's important news stories.","airtime":"SAT 1:30am-2am","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/04/washington-week.jpg","officialWebsiteLink":"http://www.pbs.org/weta/washingtonweek/","meta":{"site":"news","source":"pbs"},"link":"/radio/program/washington-week","subscribe":{"apple":"https://itunes.apple.com/us/podcast/washington-week-audio-pbs/id83324702?mt=2","tuneIn":"https://tunein.com/podcasts/Current-Affairs/Washington-Week-p693/","rss":"http://feeds.pbs.org/pbs/weta/washingtonweek-audio"}},"weekend-edition-saturday":{"id":"weekend-edition-saturday","title":"Weekend Edition Saturday","info":"Weekend Edition Saturday wraps up the week's news and offers a mix of analysis and features on a wide range of topics, including arts, sports, entertainment, and human interest stories. The two-hour program is hosted by NPR's Peabody Award-winning Scott Simon.","airtime":"SAT 5am-10am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Weekend-Edition-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.npr.org/programs/weekend-edition-saturday/","meta":{"site":"news","source":"npr"},"link":"/radio/program/weekend-edition-saturday"},"weekend-edition-sunday":{"id":"weekend-edition-sunday","title":"Weekend Edition Sunday","info":"Weekend Edition Sunday features interviews with newsmakers, artists, scientists, politicians, musicians, writers, theologians and historians. The program has covered news events from Nelson Mandela's 1990 release from a South African prison to the capture of Saddam Hussein.","airtime":"SUN 5am-10am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Weekend-Edition-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.npr.org/programs/weekend-edition-sunday/","meta":{"site":"news","source":"npr"},"link":"/radio/program/weekend-edition-sunday"},"world-affairs":{"id":"world-affairs","title":"World Affairs","info":"The world as we knew it is undergoing a rapid transformation…so what's next? Welcome to WorldAffairs, your guide to a changing world. We give you the context you need to navigate across borders and ideologies. Through sound-rich stories and in-depth interviews, we break down what it means to be a global citizen on a hot, crowded planet. Our hosts, Ray Suarez, Teresa Cotsirilos and Philip Yun help you make sense of an uncertain world, one story at a time.","airtime":"MON 10pm, TUE 1am, SAT 3am","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/World-Affairs-Podcast-Tile-360x360-1.jpg ","officialWebsiteLink":"https://www.worldaffairs.org/","meta":{"site":"news","source":"World Affairs"},"link":"/radio/program/world-affairs","subscribe":{"apple":"https://itunes.apple.com/us/podcast/world-affairs/id101215657?mt=2","tuneIn":"https://tunein.com/radio/WorldAffairs-p1665/","rss":"https://worldaffairs.libsyn.com/rss"}},"on-shifting-ground":{"id":"on-shifting-ground","title":"On Shifting Ground with Ray Suarez","info":"Geopolitical turmoil. A warming planet. Authoritarians on the rise. We live in a chaotic world that’s rapidly shifting around us. “On Shifting Ground with Ray Suarez” explores international fault lines and how they impact us all. Each week, NPR veteran Ray Suarez hosts conversations with journalists, leaders and policy experts to help us read between the headlines – and give us hope for human resilience.","airtime":"MON 10pm, TUE 1am, SAT 3am","imageSrc":"https://ww2.kqed.org/app/uploads/2022/12/onshiftingground-600x600-1.png","officialWebsiteLink":"https://worldaffairs.org/radio-podcast/","meta":{"site":"news","source":"On Shifting Ground"},"link":"/radio/program/on-shifting-ground","subscribe":{"apple":"https://podcasts.apple.com/ie/podcast/on-shifting-ground/id101215657","rss":"https://feeds.libsyn.com/36668/rss"}},"hidden-brain":{"id":"hidden-brain","title":"Hidden Brain","info":"Shankar Vedantam uses science and storytelling to reveal the unconscious patterns that drive human behavior, shape our choices and direct our relationships.","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/05/hiddenbrain.jpg","officialWebsiteLink":"https://www.npr.org/series/423302056/hidden-brain","airtime":"SUN 7pm-8pm","meta":{"site":"news","source":"NPR"},"link":"/radio/program/hidden-brain","subscribe":{"apple":"https://itunes.apple.com/us/podcast/hidden-brain/id1028908750?mt=2","tuneIn":"https://tunein.com/podcasts/Science-Podcasts/Hidden-Brain-p787503/","rss":"https://feeds.npr.org/510308/podcast.xml"}},"city-arts":{"id":"city-arts","title":"City Arts & Lectures","info":"A one-hour radio program to hear celebrated writers, artists and thinkers address contemporary ideas and values, often discussing the creative process. Please note: tapes or transcripts are not available","imageSrc":"https://ww2.kqed.org/radio/wp-content/uploads/sites/50/2018/05/cityartsandlecture-300x300.jpg","officialWebsiteLink":"https://www.cityarts.net/","airtime":"SUN 1pm-2pm, TUE 10pm, WED 1am","meta":{"site":"news","source":"City Arts & Lectures"},"link":"https://www.cityarts.net","subscribe":{"tuneIn":"https://tunein.com/radio/City-Arts-and-Lectures-p692/","rss":"https://www.cityarts.net/feed/"}},"white-lies":{"id":"white-lies","title":"White Lies","info":"In 1965, Rev. James Reeb was murdered in Selma, Alabama. Three men were tried and acquitted, but no one was ever held to account. Fifty years later, two journalists from Alabama return to the city where it happened, expose the lies that kept the murder from being solved and uncover a story about guilt and memory that says as much about America today as it does about the past.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/White-Lies-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.npr.org/podcasts/510343/white-lies","meta":{"site":"news","source":"npr"},"link":"/radio/program/white-lies","subscribe":{"npr":"https://rpb3r.app.goo.gl/whitelies","apple":"https://podcasts.apple.com/podcast/id1462650519?mt=2&at=11l79Y&ct=nprdirectory","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5ucHIub3JnLzUxMDM0My9wb2RjYXN0LnhtbA","spotify":"https://open.spotify.com/show/12yZ2j8vxqhc0QZyRES3ft?si=LfWYEK6URA63hueKVxRLAw","rss":"https://feeds.npr.org/510343/podcast.xml"}},"rightnowish":{"id":"rightnowish","title":"Rightnowish","tagline":"Art is where you find it","info":"Rightnowish digs into life in the Bay Area right now… ish. Journalist Pendarvis Harshaw takes us to galleries painted on the sides of liquor stores in West Oakland. We'll dance in warehouses in the Bayview, make smoothies with kids in South Berkeley, and listen to classical music in a 1984 Cutlass Supreme in Richmond. Every week, Pen talks to movers and shakers about how the Bay Area shapes what they create, and how they shape the place we call home.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/Rightnowish-Podcast-Tile-500x500-1.jpg","imageAlt":"KQED Rightnowish with Pendarvis Harshaw","officialWebsiteLink":"/podcasts/rightnowish","meta":{"site":"arts","source":"kqed","order":"5"},"link":"/podcasts/rightnowish","subscribe":{"npr":"https://www.npr.org/podcasts/721590300/rightnowish","rss":"https://ww2.kqed.org/arts/programs/rightnowish/feed/podcast","apple":"https://podcasts.apple.com/us/podcast/rightnowish/id1482187648","stitcher":"https://www.stitcher.com/podcast/kqed/rightnowish","google":"https://podcasts.google.com/feed/aHR0cHM6Ly9mZWVkcy5tZWdhcGhvbmUuZm0vS1FJTkMxMjU5MTY3NDc4","spotify":"https://open.spotify.com/show/7kEJuafTzTVan7B78ttz1I"}},"jerrybrown":{"id":"jerrybrown","title":"The Political Mind of Jerry Brown","tagline":"Lessons from a lifetime in politics","info":"The Political Mind of Jerry Brown brings listeners the wisdom of the former Governor, Mayor, and presidential candidate. Scott Shafer interviewed Brown for more than 40 hours, covering the former governor's life and half-century in the political game – and Brown has some lessons he'd like to share. ","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-Political-Mind-of-Jerry-Brown-Podcast-Tile-703x703-1.jpg","imageAlt":"KQED The Political Mind of Jerry Brown","officialWebsiteLink":"/podcasts/jerrybrown","meta":{"site":"news","source":"kqed","order":"16"},"link":"/podcasts/jerrybrown","subscribe":{"npr":"https://www.npr.org/podcasts/790253322/the-political-mind-of-jerry-brown","apple":"https://itunes.apple.com/us/podcast/id1492194549","rss":"https://ww2.kqed.org/news/series/jerrybrown/feed/podcast/","tuneIn":"http://tun.in/pjGcK","stitcher":"https://www.stitcher.com/podcast/kqed/the-political-mind-of-jerry-brown","spotify":"https://open.spotify.com/show/54C1dmuyFyKMFttY6X2j6r?si=K8SgRCoISNK6ZbjpXrX5-w","google":"https://podcasts.google.com/feed/aHR0cHM6Ly93dzIua3FlZC5vcmcvbmV3cy9zZXJpZXMvamVycnlicm93bi9mZWVkL3BvZGNhc3Qv"}},"the-splendid-table":{"id":"the-splendid-table","title":"The Splendid Table","info":"\u003cem>The Splendid Table\u003c/em> hosts our nation's conversations about cooking, sustainability and food culture.","imageSrc":"https://cdn.kqed.org/wp-content/uploads/2024/04/The-Splendid-Table-Podcast-Tile-360x360-1.jpg","officialWebsiteLink":"https://www.splendidtable.org/","airtime":"SUN 10-11 pm","meta":{"site":"radio","source":"npr"},"link":"/radio/program/the-splendid-table"}},"racesReducer":{"5921":{"id":"5921","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 7","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":158422,"precinctsReportPercentage":98.97,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Doris Matsui","candidateIncumbent":true,"candidateParty":"D","voteCount":89456,"isWinner":true},{"candidateName":"Tom Silva","candidateIncumbent":false,"candidateParty":"R","voteCount":48920,"isWinner":true},{"candidateName":"David Mandel","candidateIncumbent":false,"candidateParty":"D","voteCount":20046,"isWinner":false}],"winnerDateTime":"2024-03-09T01:00:38.194Z"},"5922":{"id":"5922","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 8","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Rudy Recile","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true},{"candidateName":"John Garamendi","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"5924":{"id":"5924","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 10","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":185034,"precinctsReportPercentage":99.07,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Mark DeSaulnier","candidateIncumbent":true,"candidateParty":"D","voteCount":121265,"isWinner":true},{"candidateName":"Katherine Piccinini","candidateIncumbent":false,"candidateParty":"R","voteCount":34883,"isWinner":true},{"candidateName":"Nolan Chen","candidateIncumbent":false,"candidateParty":"R","voteCount":19459,"isWinner":false},{"candidateName":"Joe Sweeney","candidateIncumbent":false,"candidateParty":"NPP","voteCount":7606,"isWinner":false},{"candidateName":"Mohamed Elsherbini","candidateIncumbent":false,"candidateParty":"NPP","voteCount":1821,"isWinner":false}],"winnerDateTime":"2024-03-09T01:02:32.415Z"},"5926":{"id":"5926","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 12","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":153801,"precinctsReportPercentage":98.88,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 20, 2024","timeUpdated":"4:41 PM","source":"AP","candidates":[{"candidateName":"Lateefah Simon","candidateIncumbent":false,"candidateParty":"D","voteCount":85905,"isWinner":true},{"candidateName":"Jennifer Tran","candidateIncumbent":false,"candidateParty":"D","voteCount":22964,"isWinner":true},{"candidateName":"Tony Daysog","candidateIncumbent":false,"candidateParty":"D","voteCount":17197,"isWinner":false},{"candidateName":"Stephen Slauson","candidateIncumbent":false,"candidateParty":"R","voteCount":9699,"isWinner":false},{"candidateName":"Glenn Kaplan","candidateIncumbent":false,"candidateParty":"D","voteCount":6785,"isWinner":false},{"candidateName":"Eric Wilson","candidateIncumbent":false,"candidateParty":"D","voteCount":4243,"isWinner":false},{"candidateName":"Abdur Sikder","candidateIncumbent":false,"candidateParty":"D","voteCount":2847,"isWinner":false},{"candidateName":"Ned Nuerge","candidateIncumbent":false,"candidateParty":"R","voteCount":2532,"isWinner":false},{"candidateName":"Andre Todd","candidateIncumbent":false,"candidateParty":"D","voteCount":1629,"isWinner":false}],"winnerDateTime":"2024-03-16T00:22:36.062Z"},"5928":{"id":"5928","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 14","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":125831,"precinctsReportPercentage":99.14,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 20, 2024","timeUpdated":"4:41 PM","source":"AP","candidates":[{"candidateName":"Eric Swalwell","candidateIncumbent":true,"candidateParty":"D","voteCount":83989,"isWinner":true},{"candidateName":"Vin Kruttiventi","candidateIncumbent":false,"candidateParty":"R","voteCount":22106,"isWinner":true},{"candidateName":"Alison Hayden","candidateIncumbent":false,"candidateParty":"R","voteCount":11928,"isWinner":false},{"candidateName":"Luis Reynoso","candidateIncumbent":false,"candidateParty":"R","voteCount":7808,"isWinner":false}],"winnerDateTime":"2024-03-12T00:51:36.366Z"},"5930":{"id":"5930","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 16","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":182135,"precinctsReportPercentage":98.91,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"April 3, 2024","timeUpdated":"3:04 PM","source":"AP","candidates":[{"candidateName":"Sam Liccardo","candidateIncumbent":false,"candidateParty":"D","voteCount":38489,"isWinner":true},{"candidateName":"Evan Low","candidateIncumbent":false,"candidateParty":"D","voteCount":30249,"isWinner":false},{"candidateName":"Joe Simitian","candidateIncumbent":false,"candidateParty":"D","voteCount":30249,"isWinner":false},{"candidateName":"Peter Ohtaki","candidateIncumbent":false,"candidateParty":"R","voteCount":23275,"isWinner":false},{"candidateName":"Peter Dixon","candidateIncumbent":false,"candidateParty":"D","voteCount":14673,"isWinner":false},{"candidateName":"Rishi Kumar","candidateIncumbent":false,"candidateParty":"D","voteCount":12377,"isWinner":false},{"candidateName":"Karl Ryan","candidateIncumbent":false,"candidateParty":"R","voteCount":11557,"isWinner":false},{"candidateName":"Julie Lythcott-Haims","candidateIncumbent":false,"candidateParty":"D","voteCount":11383,"isWinner":false},{"candidateName":"Ahmed Mostafa","candidateIncumbent":false,"candidateParty":"D","voteCount":5811,"isWinner":false},{"candidateName":"Greg Tanaka","candidateIncumbent":false,"candidateParty":"D","voteCount":2421,"isWinner":false},{"candidateName":"Joby Bernstein","candidateIncumbent":false,"candidateParty":"D","voteCount":1651,"isWinner":false}],"winnerDateTime":"2024-03-12T00:32:05.002Z"},"5931":{"id":"5931","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 17","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":117534,"precinctsReportPercentage":98.92,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Ro Khanna","candidateIncumbent":true,"candidateParty":"D","voteCount":73941,"isWinner":true},{"candidateName":"Anita Chen","candidateIncumbent":false,"candidateParty":"R","voteCount":31539,"isWinner":true},{"candidateName":"Ritesh Tandon","candidateIncumbent":false,"candidateParty":"D","voteCount":5728,"isWinner":false},{"candidateName":"Mario Ramirez","candidateIncumbent":false,"candidateParty":"D","voteCount":4491,"isWinner":false},{"candidateName":"Joe Dehn","candidateIncumbent":false,"candidateParty":"Lib","voteCount":1835,"isWinner":false}],"winnerDateTime":"2024-03-08T01:50:53.956Z"},"5932":{"id":"5932","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 18","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":96302,"precinctsReportPercentage":98.93,"eevp":98.83,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Zoe Lofgren","candidateIncumbent":true,"candidateParty":"D","voteCount":49323,"isWinner":true},{"candidateName":"Peter Hernandez","candidateIncumbent":false,"candidateParty":"R","voteCount":31622,"isWinner":true},{"candidateName":"Charlene Nijmeh","candidateIncumbent":false,"candidateParty":"D","voteCount":10614,"isWinner":false},{"candidateName":"Lawrence Milan","candidateIncumbent":false,"candidateParty":"D","voteCount":2712,"isWinner":false},{"candidateName":"Luele Kifle","candidateIncumbent":false,"candidateParty":"D","voteCount":2031,"isWinner":false}],"winnerDateTime":"2024-03-12T00:26:02.706Z"},"5963":{"id":"5963","type":"apRace","location":"State of California","raceName":"State House, District 2","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":139085,"precinctsReportPercentage":98.62,"eevp":98.6,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Michael Greer","candidateIncumbent":false,"candidateParty":"R","voteCount":38079,"isWinner":true},{"candidateName":"Chris Rogers","candidateIncumbent":false,"candidateParty":"D","voteCount":27126,"isWinner":true},{"candidateName":"Rusty Hicks","candidateIncumbent":false,"candidateParty":"D","voteCount":25615,"isWinner":false},{"candidateName":"Ariel Kelley","candidateIncumbent":false,"candidateParty":"D","voteCount":19483,"isWinner":false},{"candidateName":"Frankie Myers","candidateIncumbent":false,"candidateParty":"D","voteCount":17694,"isWinner":false},{"candidateName":"Ted Williams","candidateIncumbent":false,"candidateParty":"D","voteCount":9550,"isWinner":false},{"candidateName":"Cynthia Click","candidateIncumbent":false,"candidateParty":"D","voteCount":1538,"isWinner":false}],"winnerDateTime":"2024-03-22T21:38:36.711Z"},"5972":{"id":"5972","type":"apRace","location":"State of California","raceName":"State House, District 11","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":99775,"precinctsReportPercentage":99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Lori Wilson","candidateIncumbent":true,"candidateParty":"D","voteCount":50085,"isWinner":true},{"candidateName":"Dave Ennis","candidateIncumbent":false,"candidateParty":"R","voteCount":26074,"isWinner":true},{"candidateName":"Wanda Wallis","candidateIncumbent":false,"candidateParty":"R","voteCount":14638,"isWinner":false},{"candidateName":"Jeffrey Flack","candidateIncumbent":false,"candidateParty":"D","voteCount":8978,"isWinner":false}],"winnerDateTime":"2024-03-08T02:01:24.524Z"},"5973":{"id":"5973","type":"apRace","location":"State of California","raceName":"State House, District 12","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":143532,"precinctsReportPercentage":99.19,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:38 PM","source":"AP","candidates":[{"candidateName":"Damon Connolly","candidateIncumbent":true,"candidateParty":"D","voteCount":111275,"isWinner":true},{"candidateName":"Andy Podshadley","candidateIncumbent":false,"candidateParty":"R","voteCount":17240,"isWinner":true},{"candidateName":"Eryn Cervantes","candidateIncumbent":false,"candidateParty":"R","voteCount":15017,"isWinner":false}],"winnerDateTime":"2024-03-21T00:25:32.262Z"},"5975":{"id":"5975","type":"apRace","location":"State of California","raceName":"State House, District 14","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":106997,"precinctsReportPercentage":99.06,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Buffy Wicks","candidateIncumbent":true,"candidateParty":"D","voteCount":78678,"isWinner":true},{"candidateName":"Margot Smith","candidateIncumbent":false,"candidateParty":"D","voteCount":18251,"isWinner":true},{"candidateName":"Utkarsh Jain","candidateIncumbent":false,"candidateParty":"R","voteCount":10068,"isWinner":false}],"winnerDateTime":"2024-03-15T01:30:34.539Z"},"5976":{"id":"5976","type":"apRace","location":"State of California","raceName":"State House, District 15","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":97144,"precinctsReportPercentage":98.98,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Sonia Ledo","candidateIncumbent":false,"candidateParty":"R","voteCount":30946,"isWinner":true},{"candidateName":"Anamarie Farias","candidateIncumbent":false,"candidateParty":"D","voteCount":29512,"isWinner":true},{"candidateName":"Monica Wilson","candidateIncumbent":false,"candidateParty":"D","voteCount":24775,"isWinner":false},{"candidateName":"Karen Mitchoff","candidateIncumbent":false,"candidateParty":"D","voteCount":11911,"isWinner":false}],"winnerDateTime":"2024-03-14T00:19:38.858Z"},"5977":{"id":"5977","type":"apRace","location":"State of California","raceName":"State House, District 16","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Joseph Rubay","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true},{"candidateName":"Rebecca Bauer-Kahan","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"5978":{"id":"5978","type":"apRace","location":"State of California","raceName":"State House, District 17","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":111003,"precinctsReportPercentage":98.99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"8:25 AM","source":"AP","candidates":[{"candidateName":"Matt Haney","candidateIncumbent":true,"candidateParty":"D","voteCount":90915,"isWinner":true},{"candidateName":"Manuel Noris-Barrera","candidateIncumbent":false,"candidateParty":"R","voteCount":13843,"isWinner":true},{"candidateName":"Otto Duke","candidateIncumbent":false,"candidateParty":"D","voteCount":6245,"isWinner":false}],"winnerDateTime":"2024-03-12T00:36:19.697Z"},"5979":{"id":"5979","type":"apRace","location":"State of California","raceName":"State House, District 18","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":86008,"precinctsReportPercentage":99.1,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 20, 2024","timeUpdated":"4:41 PM","source":"AP","candidates":[{"candidateName":"Mia Bonta","candidateIncumbent":true,"candidateParty":"D","voteCount":73040,"isWinner":true},{"candidateName":"Andre Sandford","candidateIncumbent":false,"candidateParty":"AIP","voteCount":4575,"isWinner":false},{"candidateName":"Mindy Pechenuk","candidateIncumbent":false,"candidateParty":"R","voteCount":4389,"isWinner":false},{"candidateName":"Cheyenne Kenney","candidateIncumbent":false,"candidateParty":"R","voteCount":4004,"isWinner":false}],"winnerDateTime":"2024-03-06T08:03:23.729Z"},"5980":{"id":"5980","type":"apRace","location":"State of California","raceName":"State House, District 19","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":113959,"precinctsReportPercentage":98.8,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Catherine Stefani","candidateIncumbent":false,"candidateParty":"D","voteCount":64960,"isWinner":true},{"candidateName":"David Lee","candidateIncumbent":false,"candidateParty":"D","voteCount":33035,"isWinner":true},{"candidateName":"Nadia Flamenco","candidateIncumbent":false,"candidateParty":"R","voteCount":8335,"isWinner":false},{"candidateName":"Arjun Sodhani","candidateIncumbent":false,"candidateParty":"R","voteCount":7629,"isWinner":false}],"winnerDateTime":"2024-03-11T23:50:23.109Z"},"5981":{"id":"5981","type":"apRace","location":"State of California","raceName":"State House, District 20","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 20, 2024","timeUpdated":"4:36 PM","source":"AP","candidates":[{"candidateName":"Liz Ortega","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"5982":{"id":"5982","type":"apRace","location":"State of California","raceName":"State House, District 21","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Mark Gilham","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true},{"candidateName":"Diane Papan","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"5984":{"id":"5984","type":"apRace","location":"State of California","raceName":"State House, District 23","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":116963,"precinctsReportPercentage":98.91,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Marc Berman","candidateIncumbent":true,"candidateParty":"D","voteCount":67106,"isWinner":true},{"candidateName":"Lydia Kou","candidateIncumbent":false,"candidateParty":"D","voteCount":23699,"isWinner":true},{"candidateName":"Gus Mattammal","candidateIncumbent":false,"candidateParty":"R","voteCount":13277,"isWinner":false},{"candidateName":"Allan Marson","candidateIncumbent":false,"candidateParty":"R","voteCount":12881,"isWinner":false}],"winnerDateTime":"2024-03-12T01:13:06.280Z"},"5987":{"id":"5987","type":"apRace","location":"State of California","raceName":"State House, District 26","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":72753,"precinctsReportPercentage":99.19,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Patrick Ahrens","candidateIncumbent":false,"candidateParty":"D","voteCount":25036,"isWinner":true},{"candidateName":"Tara Sreekrishnan","candidateIncumbent":false,"candidateParty":"D","voteCount":19600,"isWinner":true},{"candidateName":"Sophie Song","candidateIncumbent":false,"candidateParty":"R","voteCount":15954,"isWinner":false},{"candidateName":"Omar Din","candidateIncumbent":false,"candidateParty":"D","voteCount":8772,"isWinner":false},{"candidateName":"Bob Goodwyn","candidateIncumbent":false,"candidateParty":"Lib","voteCount":2170,"isWinner":false},{"candidateName":"Ashish Garg","candidateIncumbent":false,"candidateParty":"NPP","voteCount":1221,"isWinner":false}],"winnerDateTime":"2024-03-13T21:06:29.070Z"},"5989":{"id":"5989","type":"apRace","location":"State of California","raceName":"State House, District 28","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"5:10 PM","source":"AP","candidates":[{"candidateName":"Gail Pellerin","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true},{"candidateName":"Liz Lawler","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6010":{"id":"6010","type":"apRace","location":"State of California","raceName":"State House, District 49","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:36 PM","source":"AP","candidates":[{"candidateName":"Mike Fong","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true},{"candidateName":"Long Liu","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6018":{"id":"6018","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 2","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":229348,"precinctsReportPercentage":99.05,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:38 PM","source":"AP","candidates":[{"candidateName":"Jared Huffman","candidateIncumbent":true,"candidateParty":"D","voteCount":169005,"isWinner":true},{"candidateName":"Chris Coulombe","candidateIncumbent":false,"candidateParty":"R","voteCount":37372,"isWinner":true},{"candidateName":"Tief Gibbs","candidateIncumbent":false,"candidateParty":"R","voteCount":18437,"isWinner":false},{"candidateName":"Jolian Kangas","candidateIncumbent":false,"candidateParty":"NPP","voteCount":3166,"isWinner":false},{"candidateName":"Jason Brisendine","candidateIncumbent":false,"candidateParty":"NPP","voteCount":1368,"isWinner":false}],"winnerDateTime":"2024-03-12T00:46:10.103Z"},"6020":{"id":"6020","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 4","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":187640,"precinctsReportPercentage":96.32,"eevp":96.36,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Mike Thompson","candidateIncumbent":true,"candidateParty":"D","voteCount":118147,"isWinner":true},{"candidateName":"John Munn","candidateIncumbent":false,"candidateParty":"R","voteCount":56232,"isWinner":true},{"candidateName":"Andrew Engdahl","candidateIncumbent":false,"candidateParty":"D","voteCount":11202,"isWinner":false},{"candidateName":"Niket Patwardhan","candidateIncumbent":false,"candidateParty":"NPP","voteCount":2059,"isWinner":false}],"winnerDateTime":"2024-03-07T00:30:57.980Z"},"6025":{"id":"6025","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 9","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":121271,"precinctsReportPercentage":99.17,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"5:10 PM","source":"AP","candidates":[{"candidateName":"Josh Harder","candidateIncumbent":true,"candidateParty":"D","voteCount":60396,"isWinner":true},{"candidateName":"Kevin Lincoln","candidateIncumbent":false,"candidateParty":"R","voteCount":36346,"isWinner":true},{"candidateName":"John McBride","candidateIncumbent":false,"candidateParty":"R","voteCount":15525,"isWinner":false},{"candidateName":"Khalid Jafri","candidateIncumbent":false,"candidateParty":"R","voteCount":9004,"isWinner":false}],"winnerDateTime":"2024-03-12T00:49:44.113Z"},"6031":{"id":"6031","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 15","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Anna Kramer","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true},{"candidateName":"Kevin Mullin","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6035":{"id":"6035","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 19","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":203670,"precinctsReportPercentage":99.11,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Jimmy Panetta","candidateIncumbent":true,"candidateParty":"D","voteCount":132540,"isWinner":true},{"candidateName":"Jason Anderson","candidateIncumbent":false,"candidateParty":"R","voteCount":58120,"isWinner":true},{"candidateName":"Sean Dougherty","candidateIncumbent":false,"candidateParty":"Grn","voteCount":13010,"isWinner":false}],"winnerDateTime":"2024-03-07T00:23:46.779Z"},"6066":{"id":"6066","type":"apRace","location":"State of California","raceName":"State House, District 3","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"5:10 PM","source":"AP","candidates":[{"candidateName":"Jamie Gallagher","candidateIncumbent":true,"candidateParty":"R","voteCount":0,"isWinner":true},{"candidateName":"Aaron Draper","candidateIncumbent":false,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6067":{"id":"6067","type":"apRace","location":"State of California","raceName":"State House, District 4","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Cecilia Aguiar-Curry","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6087":{"id":"6087","type":"apRace","location":"State of California","raceName":"State House, District 24","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":66643,"precinctsReportPercentage":99.19,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Alex Lee","candidateIncumbent":true,"candidateParty":"D","voteCount":45544,"isWinner":true},{"candidateName":"Bob Brunton","candidateIncumbent":false,"candidateParty":"R","voteCount":14951,"isWinner":true},{"candidateName":"Marti Souza","candidateIncumbent":false,"candidateParty":"R","voteCount":6148,"isWinner":false}],"winnerDateTime":"2024-03-14T23:23:49.770Z"},"6088":{"id":"6088","type":"apRace","location":"State of California","raceName":"State House, District 25","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":69560,"precinctsReportPercentage":99.31,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Ash Kalra","candidateIncumbent":true,"candidateParty":"D","voteCount":35821,"isWinner":true},{"candidateName":"Ted Stroll","candidateIncumbent":false,"candidateParty":"R","voteCount":18255,"isWinner":true},{"candidateName":"Lan Ngo","candidateIncumbent":false,"candidateParty":"D","voteCount":15484,"isWinner":false}],"winnerDateTime":"2024-03-14T02:40:57.200Z"},"6092":{"id":"6092","type":"apRace","location":"State of California","raceName":"State House, District 29","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Robert Rivas","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true},{"candidateName":"J.W. Paine","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6223":{"id":"6223","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 46","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"5:16 PM","source":"AP","candidates":[{"candidateName":"Lou Correa","candidateIncumbent":true,"candidateParty":"D","voteCount":0,"isWinner":true},{"candidateName":"David Pan","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6530":{"id":"6530","type":"apRace","location":"State of California","raceName":"State Senate, District 3","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":222193,"precinctsReportPercentage":98.99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Thom Bogue","candidateIncumbent":false,"candidateParty":"R","voteCount":61776,"isWinner":true},{"candidateName":"Christopher Cabaldon","candidateIncumbent":false,"candidateParty":"D","voteCount":59041,"isWinner":true},{"candidateName":"Rozzana Verder-Aliga","candidateIncumbent":false,"candidateParty":"D","voteCount":45546,"isWinner":false},{"candidateName":"Jackie Elward","candidateIncumbent":false,"candidateParty":"D","voteCount":41127,"isWinner":false},{"candidateName":"Jimih Jones","candidateIncumbent":false,"candidateParty":"R","voteCount":14703,"isWinner":false}],"winnerDateTime":"2024-03-15T01:24:31.539Z"},"6531":{"id":"6531","type":"apRace","location":"State of California","raceName":"State Senate, District 5","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":171623,"precinctsReportPercentage":99.09,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"5:10 PM","source":"AP","candidates":[{"candidateName":"Jim Shoemaker","candidateIncumbent":false,"candidateParty":"R","voteCount":74935,"isWinner":true},{"candidateName":"Jerry McNerney","candidateIncumbent":false,"candidateParty":"D","voteCount":57040,"isWinner":true},{"candidateName":"Carlos Villapudua","candidateIncumbent":false,"candidateParty":"D","voteCount":39648,"isWinner":false}],"winnerDateTime":"2024-03-13T20:07:46.382Z"},"6532":{"id":"6532","type":"apRace","location":"State of California","raceName":"State Senate, District 7","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":192446,"precinctsReportPercentage":98.72,"eevp":98.78,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:48 PM","source":"AP","candidates":[{"candidateName":"Jesse Arreguín","candidateIncumbent":false,"candidateParty":"D","voteCount":61837,"isWinner":true},{"candidateName":"Jovanka Beckles","candidateIncumbent":false,"candidateParty":"D","voteCount":34025,"isWinner":true},{"candidateName":"Dan Kalb","candidateIncumbent":false,"candidateParty":"D","voteCount":28842,"isWinner":false},{"candidateName":"Kathryn Lybarger","candidateIncumbent":false,"candidateParty":"D","voteCount":28041,"isWinner":false},{"candidateName":"Sandre Swanson","candidateIncumbent":false,"candidateParty":"D","voteCount":22862,"isWinner":false},{"candidateName":"Jeanne Solnordal","candidateIncumbent":false,"candidateParty":"R","voteCount":16839,"isWinner":false}],"winnerDateTime":"2024-03-16T00:58:11.533Z"},"6533":{"id":"6533","type":"apRace","location":"State of California","raceName":"State Senate, District 9","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Tim Grayson","candidateIncumbent":false,"candidateParty":"D","voteCount":0,"isWinner":true},{"candidateName":"Marisol Rubio","candidateIncumbent":false,"candidateParty":"D","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6534":{"id":"6534","type":"apRace","location":"State of California","raceName":"State Senate, District 11","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":228260,"precinctsReportPercentage":99.09,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Scott Wiener","candidateIncumbent":true,"candidateParty":"D","voteCount":166592,"isWinner":true},{"candidateName":"Yvette Corkrean","candidateIncumbent":false,"candidateParty":"R","voteCount":34438,"isWinner":true},{"candidateName":"Cynthia Cravens","candidateIncumbent":false,"candidateParty":"D","voteCount":18513,"isWinner":false},{"candidateName":"Jing Xiong","candidateIncumbent":false,"candidateParty":"NPP","voteCount":8717,"isWinner":false}],"winnerDateTime":"2024-03-12T02:01:51.597Z"},"6535":{"id":"6535","type":"apRace","location":"State of California","raceName":"State Senate, District 13","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":227191,"precinctsReportPercentage":98.88,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Josh Becker","candidateIncumbent":true,"candidateParty":"D","voteCount":167127,"isWinner":true},{"candidateName":"Alexander Glew","candidateIncumbent":false,"candidateParty":"R","voteCount":42788,"isWinner":true},{"candidateName":"Christina Laskowski","candidateIncumbent":false,"candidateParty":"R","voteCount":17276,"isWinner":false}],"winnerDateTime":"2024-03-12T01:56:24.964Z"},"6536":{"id":"6536","type":"apRace","location":"State of California","raceName":"State Senate, District 15","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":180231,"precinctsReportPercentage":98.81,"eevp":98.95,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"4:20 PM","source":"AP","candidates":[{"candidateName":"Dave Cortese","candidateIncumbent":true,"candidateParty":"D","voteCount":124440,"isWinner":true},{"candidateName":"Robert Howell","candidateIncumbent":false,"candidateParty":"R","voteCount":34173,"isWinner":true},{"candidateName":"Tony Loaiza","candidateIncumbent":false,"candidateParty":"R","voteCount":21618,"isWinner":false}],"winnerDateTime":"2024-03-13T01:15:45.365Z"},"6548":{"id":"6548","type":"apRace","location":"State of California","raceName":"State Senate, District 39","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":0,"uncontested":true,"precinctsReportPercentage":0,"eevp":0,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 20, 2024","timeUpdated":"4:55 PM","source":"AP","candidates":[{"candidateName":"Akilah Weber","candidateIncumbent":false,"candidateParty":"D","voteCount":0,"isWinner":true},{"candidateName":"Bob Divine","candidateIncumbent":false,"candidateParty":"R","voteCount":0,"isWinner":true}],"winnerDateTime":"2024-03-06T04:00:30.000Z"},"6611":{"id":"6611","type":"apRace","location":"State of California","raceName":"U.S. House of Representatives, District 11","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":188732,"precinctsReportPercentage":98.89,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 22, 2024","timeUpdated":"8:25 AM","source":"AP","candidates":[{"candidateName":"Nancy Pelosi","candidateIncumbent":true,"candidateParty":"D","voteCount":138285,"isWinner":true},{"candidateName":"Bruce Lou","candidateIncumbent":false,"candidateParty":"R","voteCount":16285,"isWinner":true},{"candidateName":"Marjorie Mikels","candidateIncumbent":false,"candidateParty":"D","voteCount":9363,"isWinner":false},{"candidateName":"Bianca Von Krieg","candidateIncumbent":false,"candidateParty":"D","voteCount":7634,"isWinner":false},{"candidateName":"Jason Zeng","candidateIncumbent":false,"candidateParty":"R","voteCount":6607,"isWinner":false},{"candidateName":"Jason Boyce","candidateIncumbent":false,"candidateParty":"D","voteCount":4325,"isWinner":false},{"candidateName":"Larry Nichelson","candidateIncumbent":false,"candidateParty":"R","voteCount":3482,"isWinner":false},{"candidateName":"Eve Del Castello","candidateIncumbent":false,"candidateParty":"R","voteCount":2751,"isWinner":false}],"winnerDateTime":"2024-03-12T00:31:55.445Z"},"8589":{"id":"8589","type":"apRace","location":"State of California","raceName":"U.S. Senate, Class I","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":7276537,"precinctsReportPercentage":99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Adam Schiff","candidateIncumbent":false,"candidateParty":"D","voteCount":2299507,"isWinner":true},{"candidateName":"Steve Garvey","candidateIncumbent":false,"candidateParty":"R","voteCount":2292414,"isWinner":true},{"candidateName":"Katie Porter","candidateIncumbent":false,"candidateParty":"D","voteCount":1115606,"isWinner":false},{"candidateName":"Barbara Lee","candidateIncumbent":false,"candidateParty":"D","voteCount":714408,"isWinner":false},{"candidateName":"Eric Early","candidateIncumbent":false,"candidateParty":"R","voteCount":240723,"isWinner":false},{"candidateName":"James Bradley","candidateIncumbent":false,"candidateParty":"R","voteCount":98180,"isWinner":false},{"candidateName":"Christina Pascucci","candidateIncumbent":false,"candidateParty":"D","voteCount":61755,"isWinner":false},{"candidateName":"Sharleta Bassett","candidateIncumbent":false,"candidateParty":"R","voteCount":54422,"isWinner":false},{"candidateName":"Sarah Liew","candidateIncumbent":false,"candidateParty":"R","voteCount":38483,"isWinner":false},{"candidateName":"Laura Garza ","candidateIncumbent":false,"candidateParty":"NPP","voteCount":34320,"isWinner":false},{"candidateName":"Jonathan Reiss","candidateIncumbent":false,"candidateParty":"R","voteCount":34283,"isWinner":false},{"candidateName":"Sepi Gilani","candidateIncumbent":false,"candidateParty":"D","voteCount":34056,"isWinner":false},{"candidateName":"Gail Lightfoot","candidateIncumbent":false,"candidateParty":"Lib","voteCount":33046,"isWinner":false},{"candidateName":"Denice Gary-Pandol","candidateIncumbent":false,"candidateParty":"R","voteCount":25494,"isWinner":false},{"candidateName":"James Macauley","candidateIncumbent":false,"candidateParty":"R","voteCount":23168,"isWinner":false},{"candidateName":"Harmesh Kumar","candidateIncumbent":false,"candidateParty":"D","voteCount":21522,"isWinner":false},{"candidateName":"David Peterson","candidateIncumbent":false,"candidateParty":"D","voteCount":21076,"isWinner":false},{"candidateName":"Douglas Pierce","candidateIncumbent":false,"candidateParty":"D","voteCount":19371,"isWinner":false},{"candidateName":"Major Singh","candidateIncumbent":false,"candidateParty":"NPP","voteCount":16965,"isWinner":false},{"candidateName":"John Rose","candidateIncumbent":false,"candidateParty":"D","voteCount":14577,"isWinner":false},{"candidateName":"Perry Pound","candidateIncumbent":false,"candidateParty":"D","voteCount":14134,"isWinner":false},{"candidateName":"Raji Rab","candidateIncumbent":false,"candidateParty":"D","voteCount":13558,"isWinner":false},{"candidateName":"Mark Ruzon","candidateIncumbent":false,"candidateParty":"NPP","voteCount":13429,"isWinner":false},{"candidateName":"Forrest Jones","candidateIncumbent":false,"candidateParty":"AIP","voteCount":13027,"isWinner":false},{"candidateName":"Stefan Simchowitz","candidateIncumbent":false,"candidateParty":"R","voteCount":12717,"isWinner":false},{"candidateName":"Martin Veprauskas","candidateIncumbent":false,"candidateParty":"R","voteCount":9714,"isWinner":false},{"candidateName":"Don Grundmann","candidateIncumbent":false,"candidateParty":"NPP","voteCount":6582,"isWinner":false}],"winnerDateTime":"2024-03-06T05:01:46.589Z"},"8686":{"id":"8686","type":"apRace","location":"State of California","raceName":"President,","raceDescription":"Top candidate wins seat.","raceType":"top1","totalVotes":3589127,"precinctsReportPercentage":99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:48 AM","source":"AP","candidates":[{"candidateName":"Joe Biden","candidateIncumbent":true,"candidateParty":"D","voteCount":3200188,"isWinner":true},{"candidateName":"Marianne Williamson","candidateIncumbent":false,"candidateParty":"D","voteCount":145690,"isWinner":false},{"candidateName":"Dean Phillips","candidateIncumbent":false,"candidateParty":"D","voteCount":99981,"isWinner":false},{"candidateName":"Armando Perez-Serrato","candidateIncumbent":false,"candidateParty":"D","voteCount":42925,"isWinner":false},{"candidateName":"Gabriel Cornejo","candidateIncumbent":false,"candidateParty":"D","voteCount":41261,"isWinner":false},{"candidateName":"President Boddie","candidateIncumbent":false,"candidateParty":"D","voteCount":25373,"isWinner":false},{"candidateName":"Stephen Lyons","candidateIncumbent":false,"candidateParty":"D","voteCount":21008,"isWinner":false},{"candidateName":"Eban Cambridge","candidateIncumbent":false,"candidateParty":"D","voteCount":12701,"isWinner":false}],"winnerDateTime":"2024-03-06T04:12:27.559Z"},"8688":{"id":"8688","type":"apRace","location":"State of California","raceName":"President,","raceDescription":"Top candidate wins seat.","raceType":"top1","totalVotes":2466569,"precinctsReportPercentage":99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Donald Trump","candidateIncumbent":false,"candidateParty":"R","voteCount":1953947,"isWinner":true},{"candidateName":"Nikki Haley","candidateIncumbent":false,"candidateParty":"R","voteCount":430792,"isWinner":false},{"candidateName":"Ron DeSantis","candidateIncumbent":false,"candidateParty":"R","voteCount":35581,"isWinner":false},{"candidateName":"Chris Christie","candidateIncumbent":false,"candidateParty":"R","voteCount":20164,"isWinner":false},{"candidateName":"Vivek Ramaswamy","candidateIncumbent":false,"candidateParty":"R","voteCount":11069,"isWinner":false},{"candidateName":"Rachel Swift","candidateIncumbent":false,"candidateParty":"R","voteCount":4231,"isWinner":false},{"candidateName":"David Stuckenberg","candidateIncumbent":false,"candidateParty":"R","voteCount":3895,"isWinner":false},{"candidateName":"Ryan Binkley","candidateIncumbent":false,"candidateParty":"R","voteCount":3563,"isWinner":false},{"candidateName":"Asa Hutchinson","candidateIncumbent":false,"candidateParty":"R","voteCount":3327,"isWinner":false}],"winnerDateTime":"2024-03-06T04:13:19.766Z"},"81993":{"id":"81993","type":"apRace","location":"State of California","raceName":"U.S. Senate, Class I Unexpired Term","raceDescription":"Top candidate wins seat.","raceType":"top2","totalVotes":7358837,"precinctsReportPercentage":99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Steve Garvey","candidateIncumbent":false,"candidateParty":"R","voteCount":2444940,"isWinner":true},{"candidateName":"Adam Schiff","candidateIncumbent":false,"candidateParty":"D","voteCount":2155146,"isWinner":true},{"candidateName":"Katie Porter","candidateIncumbent":false,"candidateParty":"D","voteCount":1269194,"isWinner":false},{"candidateName":"Barbara Lee","candidateIncumbent":false,"candidateParty":"D","voteCount":863278,"isWinner":false},{"candidateName":"Eric Early","candidateIncumbent":false,"candidateParty":"R","voteCount":448788,"isWinner":false},{"candidateName":"Christina Pascucci","candidateIncumbent":false,"candidateParty":"D","voteCount":109421,"isWinner":false},{"candidateName":"Sepi Gilani","candidateIncumbent":false,"candidateParty":"D","voteCount":68070,"isWinner":false}],"winnerDateTime":"2024-03-06T04:31:08.186Z"},"82014":{"id":"82014","type":"apRace","location":"State of California","raceName":"Proposition, 1 - Behavioral Health Services Program","raceDescription":"Top candidate wins seat.","raceType":"top1","totalVotes":7221972,"precinctsReportPercentage":99,"eevp":99,"tabulationStatus":"Tabulation Paused","dateUpdated":"March 25, 2024","timeUpdated":"5:47 AM","source":"AP","candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":null,"voteCount":3624998,"isWinner":true},{"candidateName":"No","candidateIncumbent":false,"candidateParty":null,"voteCount":3596974,"isWinner":false}],"winnerDateTime":"2024-03-21T00:11:06.265Z"},"timeLoaded":"April 18, 2024 8:23 AM","nationalRacesLoaded":true,"localRacesLoaded":true,"overrides":[{"id":"5921","raceName":"U.S. House of Representatives, District 7","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5922","raceName":"U.S. House of Representatives, District 8","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5924","raceName":"U.S. House of Representatives, District 10","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5926","raceName":"U.S. House of Representatives, District 12","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/alameda/congress-12th-district"},{"id":"5928","raceName":"U.S. House of Representatives, District 14","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5930","raceName":"U.S. House of Representatives, District 16","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/california/congress-16th-district"},{"id":"5931","raceName":"U.S. House of Representatives, District 17","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5932","raceName":"U.S. House of Representatives, District 18","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5963","raceName":"State Assembly, District 2","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5972","raceName":"State Assembly, District 11","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5973","raceName":"State Assembly, District 12","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5975","raceName":"State Assembly, District 14","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5976","raceName":"State Assembly, District 15","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/contracosta/state-assembly"},{"id":"5977","raceName":"State Assembly, District 16","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5978","raceName":"State Assembly, District 17","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5979","raceName":"State Assembly, District 18","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5980","raceName":"State Assembly, District 19","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5981","raceName":"State Assembly, District 20","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5982","raceName":"State Assembly, District 21","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"5984","raceName":"State Assembly, District 23","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/california/state-assembly-23rd-district"},{"id":"5987","raceName":"State Assembly, District 26","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/santaclara/state-assembly-26th-district"},{"id":"5989","raceName":"State Assembly, District 28","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6010","raceName":"State Assembly, District 4","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6018","raceName":"U.S. House of Representatives, District 2","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6020","raceName":"U.S. House of Representatives, District 4","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6025","raceName":"U.S. House of Representatives, District 9","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6031","raceName":"U.S. House of Representatives, District 15","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6035","raceName":"U.S. House of Representatives, District 19","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6067","raceName":"State Assembly, District 4","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6087","raceName":"State Assembly, District 24","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6088","raceName":"State Assembly, District 25","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6092","raceName":"State Assembly, District 29","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6223","raceName":"U.S. House of Representatives, District 4","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6530","raceName":"State Senate, District 3","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/california/state-senate-3rd-district"},{"id":"6531","raceName":"State Senate, District 5","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6532","raceName":"State Senate, District 7","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/california/state-senate-7th-district"},{"id":"6533","raceName":"State Senate, District 9","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6534","raceName":"State Senate, District 11","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6535","raceName":"State Senate, District 13","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6536","raceName":"State Senate, District 15","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"6611","raceName":"U.S. House of Representatives, District 11","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":""},{"id":"8589","raceName":"U.S. Senate (Full Term)","raceDescription":"Top two candidates advance to general election.","raceReadTheStory":"https://www.kqed.org/elections/results/california/senator"},{"id":"8686","raceName":"California Democratic Presidential Primary","raceDescription":"Candidates are competing for 496 delegates.","raceReadTheStory":"https://www.kqed.org/elections/results/president/democrat"},{"id":"8688","raceName":"California Republican Presidential Primary","raceDescription":"Candidates are competing for 169 delegates.","raceReadTheStory":"https://kqed.org/elections/results/president/republican"},{"id":"81993","raceName":"U.S. Senate (Partial/Unexpired Term)","raceDescription":"Top two candidates advance to general election."},{"id":"82014","raceName":"Proposition 1","raceDescription":"Bond and mental health reforms. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/california/proposition-1"}],"AlamedaJudge5":{"id":"AlamedaJudge5","type":"localRace","location":"Alameda","raceName":"Superior Court Judge, Office 5","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":200601,"candidates":[{"candidateName":"Terry Wiley","candidateIncumbent":true,"candidateParty":"","voteCount":200601}]},"AlamedaJudge12":{"id":"AlamedaJudge12","type":"localRace","location":"Alameda","raceName":"Superior Court Judge, Office 12","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":240853,"candidates":[{"candidateName":"Mark Fickes","candidateIncumbent":false,"candidateParty":"","voteCount":133009},{"candidateName":"Michael P. Johnson","candidateIncumbent":false,"candidateParty":"","voteCount":107844}]},"AlamedaBoard2":{"id":"AlamedaBoard2","type":"localRace","location":"Alameda","raceName":"Board of Education, Trustee Area 2","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":33580,"candidates":[{"candidateName":"John Lewis","candidateIncumbent":false,"candidateParty":"","voteCount":6943},{"candidateName":"Angela Normand","candidateIncumbent":true,"candidateParty":"","voteCount":26637}]},"AlamedaBoard5":{"id":"AlamedaBoard5","type":"localRace","location":"Alameda","raceName":"Board of Education, Trustee Area 5","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":26072,"candidates":[{"candidateName":"Guadalupe \"Lupe\" Angulo","candidateIncumbent":false,"candidateParty":"","voteCount":7521},{"candidateName":"Janevette Cole","candidateIncumbent":true,"candidateParty":"","voteCount":13338},{"candidateName":"Joe Orlando Ramos","candidateIncumbent":false,"candidateParty":"","voteCount":5213}]},"AlamedaBoard6":{"id":"AlamedaBoard6","type":"localRace","location":"Alameda","raceName":"Board of Education, Trustee Area 6","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":30864,"candidates":[{"candidateName":"John Guerrero","candidateIncumbent":false,"candidateParty":"","voteCount":9989},{"candidateName":"Eileen McDonald","candidateIncumbent":true,"candidateParty":"","voteCount":20875}]},"AlamedaSup1":{"id":"AlamedaSup1","type":"localRace","location":"Alameda","raceName":"Board of Supervisors, District 1","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":41038,"candidates":[{"candidateName":"David Haubert","candidateIncumbent":true,"candidateParty":"","voteCount":41038}]},"AlamedaSup2":{"id":"AlamedaSup2","type":"localRace","location":"Alameda","raceName":"Board of Supervisors, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top2","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":31034,"candidates":[{"candidateName":"Elisa Márquez","candidateIncumbent":true,"candidateParty":"","voteCount":31034}]},"AlamedaSup4":{"id":"AlamedaSup4","type":"localRace","location":"Alameda","raceName":"Board of Supervisors, District 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/alameda/supervisor-4th-district","raceType":"top2","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":57007,"candidates":[{"candidateName":"Jennifer Esteen","candidateIncumbent":false,"candidateParty":"","voteCount":22400},{"candidateName":"Nate Miley","candidateIncumbent":true,"candidateParty":"","voteCount":34607}]},"AlamedaSup5":{"id":"AlamedaSup5","type":"localRace","location":"Alameda","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/alameda/supervisor-5th-district","raceType":"top2","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":81059,"candidates":[{"candidateName":"Ben Bartlett","candidateIncumbent":false,"candidateParty":"","voteCount":13518},{"candidateName":"Nikki Fortunato Bas","candidateIncumbent":false,"candidateParty":"","voteCount":27597},{"candidateName":"John J. Bauters","candidateIncumbent":false,"candidateParty":"","voteCount":16783},{"candidateName":"Ken Berrick","candidateIncumbent":false,"candidateParty":"","voteCount":7520},{"candidateName":"Omar Farmer","candidateIncumbent":false,"candidateParty":"","voteCount":1240},{"candidateName":"Gregory Hodge","candidateIncumbent":false,"candidateParty":"","voteCount":3419},{"candidateName":"Chris Moore","candidateIncumbent":false,"candidateParty":"","voteCount":7428},{"candidateName":"Gerald Pechenuk","candidateIncumbent":false,"candidateParty":"","voteCount":305},{"candidateName":"Lorrel Plimier","candidateIncumbent":false,"candidateParty":"","voteCount":3249}]},"AlamedaBoard7":{"id":"AlamedaBoard7","type":"localRace","location":"Alameda","raceName":"Flood Control & Water Conservation District Director, Zone 7, Full Term","raceDescription":"Top three candidates win seat.","raceReadTheStory":"","raceType":"top3","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":134340,"candidates":[{"candidateName":"Alan Burnham","candidateIncumbent":false,"candidateParty":"","voteCount":15723},{"candidateName":"Sandy Figuers","candidateIncumbent":false,"candidateParty":"","voteCount":22454},{"candidateName":"Laurene K. Green","candidateIncumbent":false,"candidateParty":"","voteCount":30343},{"candidateName":"Kathy Narum","candidateIncumbent":true,"candidateParty":"","voteCount":23833},{"candidateName":"Seema Badar","candidateIncumbent":false,"candidateParty":"","voteCount":7468},{"candidateName":"Catherine Brown","candidateIncumbent":false,"candidateParty":"","voteCount":34519}]},"AlamedaAuditor":{"id":"AlamedaAuditor","type":"localRace","location":"Alameda","raceName":"Oakland Auditor","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":59227,"candidates":[{"candidateName":"Michael Houston","candidateIncumbent":true,"candidateParty":"","voteCount":59227}]},"AlamedaMeasureA":{"id":"AlamedaMeasureA","type":"localRace","location":"Alameda","raceName":"Measure A","raceDescription":"Alameda County. Civil service. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":282335,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":167903},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":114432}]},"AlamedaMeasureB":{"id":"AlamedaMeasureB","type":"localRace","location":"Alameda","raceName":"Measure B","raceDescription":"Alameda County. Recall rules. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/alameda/measure-b","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":282683,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":182200},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":100483}]},"AlamedaMeasureD":{"id":"AlamedaMeasureD","type":"localRace","location":"Alameda","raceName":"Measure D","raceDescription":"Oakland. Appropriations limit. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":79797,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":59852},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":19945}]},"AlamedaMeasureE":{"id":"AlamedaMeasureE","type":"localRace","location":"Alameda","raceName":"Measure E","raceDescription":"Alameda Unified School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":22692,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":17280},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":5412}]},"AlamedaMeasureF":{"id":"AlamedaMeasureF","type":"localRace","location":"Alameda","raceName":"Measure F","raceDescription":"Piedmont. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":4855,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":3673},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":1182}]},"AlamedaMeasureG":{"id":"AlamedaMeasureG","type":"localRace","location":"Alameda","raceName":"Measure G","raceDescription":"Albany Unified School District. Parcel tax. Passes with 2/3 vote. ","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":5898,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":4651},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":1247}]},"AlamedaMeasureH":{"id":"AlamedaMeasureH","type":"localRace","location":"Alameda","raceName":"Measure H","raceDescription":"Berkeley Unified School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":33331,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":29418},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3913}]},"AlamedaMeasureI":{"id":"AlamedaMeasureI","type":"localRace","location":"Alameda","raceName":"Measure I","raceDescription":"Hayward Unified School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":21929,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":14151},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":7778}]},"AlamedaMeasureJ":{"id":"AlamedaMeasureJ","type":"localRace","location":"Alameda","raceName":"Measure J","raceDescription":"San Leandro Unified School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:02 PM","dateUpdated":"April 1, 2024","totalVotes":12338,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":7784},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":4554}]},"CCD2":{"id":"CCD2","type":"localRace","location":"Contra Costa","raceName":"Board of Supervisors, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":45776,"candidates":[{"candidateName":"Candace Andersen","candidateIncumbent":true,"candidateParty":"","voteCount":45776}]},"CCD3":{"id":"CCD3","type":"localRace","location":"Contra Costa","raceName":"Board of Supervisors, District 3","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":25120,"candidates":[{"candidateName":"Diane Burgis","candidateIncumbent":true,"candidateParty":"","voteCount":25120}]},"CCD5":{"id":"CCD5","type":"localRace","location":"Contra Costa","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/contracosta/supervisor-5th-district","raceType":"top2","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":37045,"candidates":[{"candidateName":"Mike Barbanica","candidateIncumbent":false,"candidateParty":"","voteCount":14338},{"candidateName":"Jelani Killings","candidateIncumbent":false,"candidateParty":"","voteCount":5683},{"candidateName":"Shanelle Scales-Preston","candidateIncumbent":false,"candidateParty":"","voteCount":12993},{"candidateName":"Iztaccuauhtli Hector Gonzalez","candidateIncumbent":false,"candidateParty":"","voteCount":4031}]},"CCMeasureA":{"id":"CCMeasureA","type":"localRace","location":"Contra Costa","raceName":"Measure A","raceDescription":"Martinez. Appoint City Clerk. Passes with a majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":11513,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":7554},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3959}]},"CCMeasureB":{"id":"CCMeasureB","type":"localRace","location":"Contra Costa","raceName":"Measure B","raceDescription":"Antioch Unified School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":17971,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":10397},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":7574}]},"CCMeasureC":{"id":"CCMeasureC","type":"localRace","location":"Contra Costa","raceName":"Measure C","raceDescription":"Martinez Unified School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":9230,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":6917},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":2313}]},"CCMeasureD":{"id":"CCMeasureD","type":"localRace","location":"Contra Costa","raceName":"Measure D","raceDescription":"Moraga School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:45 PM","dateUpdated":"March 28, 2024","totalVotes":6007,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":4052},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":1955}]},"MarinD2":{"id":"MarinD2","type":"localRace","location":"Marin","raceName":"Board of Supervisors, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/marin/supervisor-2nd-district","raceType":"top2","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":18466,"candidates":[{"candidateName":"Brian Colbert","candidateIncumbent":false,"candidateParty":"","voteCount":7971},{"candidateName":"Heather McPhail Sridharan","candidateIncumbent":false,"candidateParty":"","voteCount":4851},{"candidateName":"Ryan O'Neil","candidateIncumbent":false,"candidateParty":"","voteCount":2647},{"candidateName":"Gabe Paulson","candidateIncumbent":false,"candidateParty":"","voteCount":2997}]},"MarinD3":{"id":"MarinD3","type":"localRace","location":"Marin","raceName":"Board of Supervisors, District 3","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":13274,"candidates":[{"candidateName":"Stephanie Moulton-Peters","candidateIncumbent":true,"candidateParty":"","voteCount":13274}]},"MarinD4":{"id":"MarinD4","type":"localRace","location":"Marin","raceName":"Board of Supervisors, District 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":12986,"candidates":[{"candidateName":"Dennis Rodoni","candidateIncumbent":true,"candidateParty":"","voteCount":10086},{"candidateName":"Francis Drouillard","candidateIncumbent":false,"candidateParty":"","voteCount":2900}]},"MarinLarkspurCC":{"id":"MarinLarkspurCC","type":"localRace","location":"Marin","raceName":"Larkspur City Council (Short Term)","raceDescription":"Top candidate wins seat.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":4176,"candidates":[{"candidateName":"Stephanie Andre","candidateIncumbent":false,"candidateParty":"","voteCount":2514},{"candidateName":"Claire Paquette","candidateIncumbent":false,"candidateParty":"","voteCount":1008},{"candidateName":"Lana Scott","candidateIncumbent":false,"candidateParty":"","voteCount":654}]},"MarinRossCouncil":{"id":"MarinRossCouncil","type":"localRace","location":"Marin","raceName":"Ross Town Council","raceDescription":"Top three candidates win seat.","raceReadTheStory":"","raceType":"top3","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":1740,"candidates":[{"candidateName":"Charles William \"Bill\" Kircher, Jr.","candidateIncumbent":false,"candidateParty":"","voteCount":536},{"candidateName":"Mathew Salter","candidateIncumbent":false,"candidateParty":"","voteCount":502},{"candidateName":"Shadi Aboukhater","candidateIncumbent":false,"candidateParty":"","voteCount":187},{"candidateName":"Teri Dowling","candidateIncumbent":false,"candidateParty":"","voteCount":515}]},"MarinMeasureA":{"id":"MarinMeasureA","type":"localRace","location":"Marin","raceName":"Measure A","raceDescription":"Tamalpais Union High School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":45345,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":24376},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":20969}]},"MarinMeasureB":{"id":"MarinMeasureB","type":"localRace","location":"Marin","raceName":"Measure B","raceDescription":"Petaluma Joint Union High School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":132,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":62},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":70}]},"MarinMeasureC":{"id":"MarinMeasureC","type":"localRace","location":"Marin","raceName":"Measure C","raceDescription":"Belvedere. Appropriation limit. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":870,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":679},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":191}]},"MarinMeasureD":{"id":"MarinMeasureD","type":"localRace","location":"Marin","raceName":"Measure D","raceDescription":"Larkspur. Rent stabilization. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/marin/measure-d","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":4955,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":2573},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":2382}]},"MarinMeasureE":{"id":"MarinMeasureE","type":"localRace","location":"Marin","raceName":"Measure E","raceDescription":"Ross. Special tax. Passes with 2/3 vote.","raceReadTheStory":"https://www.kqed.org/elections/results/marin/measure-e","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":874,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":683},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":191}]},"MarinMeasureF":{"id":"MarinMeasureF","type":"localRace","location":"Marin","raceName":"Measure F","raceDescription":"San Anselmo. Flood Control and Water Conservation District. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":5193,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":3083},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":2110}]},"MarinMeasureG":{"id":"MarinMeasureG","type":"localRace","location":"Marin","raceName":"Measure G","raceDescription":"Bel Marin Keys Community Services District. Special tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":830,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":661},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":169}]},"MarinMeasureH":{"id":"MarinMeasureH","type":"localRace","location":"Marin","raceName":"Measure H","raceDescription":"Marinwood Community Services District. Appropriations limit, fire protection. Passes with a majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":1738,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":1369},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":369}]},"MarinMeasureI":{"id":"MarinMeasureI","type":"localRace","location":"Marin","raceName":"Measure I","raceDescription":"Marinwood Community Services District. Appropriations limit, parks. Passes with a majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:54 PM","dateUpdated":"March 27, 2024","totalVotes":1735,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":1336},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":399}]},"NapaD2":{"id":"NapaD2","type":"localRace","location":"Napa","raceName":"Board of Supervisors, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:50 PM","dateUpdated":"April 3, 2024","totalVotes":8351,"candidates":[{"candidateName":"Liz Alessio","candidateIncumbent":false,"candidateParty":"","voteCount":6340},{"candidateName":"Doris Gentry","candidateIncumbent":false,"candidateParty":"","voteCount":2011}]},"NapaD4":{"id":"NapaD4","type":"localRace","location":"Napa","raceName":"Board of Supervisors, District 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/napa/supervisor-4th-district","raceType":"top1","timeUpdated":"6:50 PM","dateUpdated":"April 3, 2024","totalVotes":7306,"candidates":[{"candidateName":"Amber Manfree","candidateIncumbent":false,"candidateParty":"","voteCount":3913},{"candidateName":"Pete Mott","candidateIncumbent":false,"candidateParty":"","voteCount":3393}]},"NapaD5":{"id":"NapaD5","type":"localRace","location":"Napa","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/napa/supervisor-5th-district","raceType":"top1","timeUpdated":"6:50 PM","dateUpdated":"April 3, 2024","totalVotes":5356,"candidates":[{"candidateName":"Mariam Aboudamous","candidateIncumbent":false,"candidateParty":"","voteCount":2379},{"candidateName":"Belia Ramos","candidateIncumbent":true,"candidateParty":"","voteCount":2977}]},"NapaMeasureD":{"id":"NapaMeasureD","type":"localRace","location":"Napa","raceName":"Measure D","raceDescription":"Howell Mountain Elementary School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"April 3, 2024","totalVotes":741,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":367},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":374}]},"NapaMeasureU":{"id":"NapaMeasureU","type":"localRace","location":"Napa","raceName":"Measure U","raceDescription":"Lake Berryessa Resort Improvement District. Appropriations limit. Passes with majority vote. ","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"April 3, 2024","totalVotes":86,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":63},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":23}]},"NapaMeasureU1":{"id":"NapaMeasureU1","type":"localRace","location":"Napa","raceName":"Measure U","raceDescription":"Yountville. Appropriations limit. Passes with majority vote. ","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"April 3, 2024","totalVotes":925,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":793},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":132}]},"SFJudge1":{"id":"SFJudge1","type":"localRace","location":"San Francisco","raceName":"Superior Court Judge, Seat 1","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/sanfrancisco/superior-court-seat-1","raceType":"top1","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":202960,"candidates":[{"candidateName":"Michael Begert","candidateIncumbent":true,"candidateParty":"","voteCount":124943},{"candidateName":"Chip Zecher","candidateIncumbent":false,"candidateParty":"","voteCount":78017}]},"SFJudge13":{"id":"SFJudge13","type":"localRace","location":"San Francisco","raceName":"Superior Court Judge, Seat 13","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/sanfrancisco/superior-court-seat-13","raceType":"top1","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":202386,"candidates":[{"candidateName":"Jean Myungjin Roland","candidateIncumbent":false,"candidateParty":"","voteCount":90012},{"candidateName":"Patrick S. Thompson","candidateIncumbent":true,"candidateParty":"","voteCount":112374}]},"SFPropA":{"id":"SFPropA","type":"localRace","location":"San Francisco","raceName":"Proposition A","raceDescription":"Housing bond. Passes with 2/3 vote.","raceReadTheStory":"https://www.kqed.org/elections/results/sanfrancisco/proposition-a","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":225187,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":158497},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":66690}]},"SFPropB":{"id":"SFPropB","type":"localRace","location":"San Francisco","raceName":"Proposition B","raceDescription":"Police staffing. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":222954,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":61580},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":161374}]},"SFPropC":{"id":"SFPropC","type":"localRace","location":"San Francisco","raceName":"Proposition C","raceDescription":"Transfer tax exemption. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":220349,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":116311},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":104038}]},"SFPropD":{"id":"SFPropD","type":"localRace","location":"San Francisco","raceName":"Proposition D","raceDescription":"Ethics laws. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":222615,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":198584},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":24031}]},"SFPropE":{"id":"SFPropE","type":"localRace","location":"San Francisco","raceName":"Proposition E","raceDescription":"Police policies. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/sanfrancisco/proposition-e","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":222817,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":120529},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":102288}]},"SFPropF":{"id":"SFPropF","type":"localRace","location":"San Francisco","raceName":"Proposition F","raceDescription":"Drug screening. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/sanfrancisco/proposition-f","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":224004,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":130214},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":93790}]},"SFPropG":{"id":"SFPropG","type":"localRace","location":"San Francisco","raceName":"Proposition G","raceDescription":"Eighth-grade algebra. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:50 PM","dateUpdated":"March 21, 2024","totalVotes":222704,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":182066},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":40638}]},"SMJudge4":{"id":"SMJudge4","type":"localRace","location":"San Mateo","raceName":"Superior Court Judge, Office 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":108919,"candidates":[{"candidateName":"Sarah Burdick","candidateIncumbent":false,"candidateParty":"","voteCount":108919}]},"SMD1":{"id":"SMD1","type":"localRace","location":"San Mateo","raceName":"Board of Supervisors, District 1","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/sanmateo/supervisor-1st-district","raceType":"top1","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":29650,"candidates":[{"candidateName":"Jackie Speier","candidateIncumbent":false,"candidateParty":"","voteCount":20353},{"candidateName":"Ann Schneider","candidateIncumbent":false,"candidateParty":"","voteCount":9297}]},"SMD4":{"id":"SMD4","type":"localRace","location":"San Mateo","raceName":"Board of Supervisors, District 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/sanmateo/supervisor-4th-district","raceType":"top2","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":22725,"candidates":[{"candidateName":"Antonio Lopez","candidateIncumbent":false,"candidateParty":"","voteCount":5730},{"candidateName":"Lisa Gauthier","candidateIncumbent":false,"candidateParty":"","voteCount":10358},{"candidateName":"Celeste Brevard","candidateIncumbent":false,"candidateParty":"","voteCount":1268},{"candidateName":"Paul Bocanegra","candidateIncumbent":false,"candidateParty":"","voteCount":1909},{"candidateName":"Maggie Cornejo","candidateIncumbent":false,"candidateParty":"","voteCount":3460}]},"SMD5":{"id":"SMD5","type":"localRace","location":"San Mateo","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":19937,"candidates":[{"candidateName":"David Canepa","candidateIncumbent":true,"candidateParty":"","voteCount":19937}]},"SMMeasureB":{"id":"SMMeasureB","type":"localRace","location":"San Mateo","raceName":"Measure B","raceDescription":"County Service Area #1 (Highlands). Special tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":1549,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":1360},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":189}]},"SMMeasureC":{"id":"SMMeasureC","type":"localRace","location":"San Mateo","raceName":"Measure C","raceDescription":"Jefferson Elementary School District. Parcel tax. Passes with 2/3 vote","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":12234,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":8543},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3691}]},"SMMeasureE":{"id":"SMMeasureE","type":"localRace","location":"San Mateo","raceName":"Measure E","raceDescription":"Woodside Elementary School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":1392,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":910},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":482}]},"SMMeasureG":{"id":"SMMeasureG","type":"localRace","location":"San Mateo","raceName":"Measure G","raceDescription":"Pacifica School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":11548,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":7067},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":4481}]},"SMMeasureH":{"id":"SMMeasureH","type":"localRace","location":"San Mateo","raceName":"Measure H","raceDescription":"San Carlos School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:56 PM","dateUpdated":"April 4, 2024","totalVotes":9938,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":6283},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3655}]},"SCJudge5":{"id":"SCJudge5","type":"localRace","location":"Santa Clara","raceName":"Superior Court Judge, Office 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":301953,"candidates":[{"candidateName":"Jay Boyarsky","candidateIncumbent":false,"candidateParty":"","voteCount":142549},{"candidateName":"Nicole M. Ford","candidateIncumbent":false,"candidateParty":"","voteCount":52147},{"candidateName":"Johnene Linda Stebbins","candidateIncumbent":false,"candidateParty":"","voteCount":107257}]},"SCD2":{"id":"SCD2","type":"localRace","location":"Santa Clara","raceName":"Board of Supervisors, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/santaclara/supervisor-2nd-district","raceType":"top2","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":44059,"candidates":[{"candidateName":"Corina Herrera-Loera","candidateIncumbent":false,"candidateParty":"","voteCount":10519},{"candidateName":"Jennifer Margaret Celaya","candidateIncumbent":false,"candidateParty":"","voteCount":2394},{"candidateName":"Madison Nguyen","candidateIncumbent":false,"candidateParty":"","voteCount":12794},{"candidateName":"Betty Duong","candidateIncumbent":false,"candidateParty":"","voteCount":14031},{"candidateName":"Nelson McElmurry","candidateIncumbent":false,"candidateParty":"","voteCount":4321}]},"SCD3":{"id":"SCD3","type":"localRace","location":"Santa Clara","raceName":"Board of Supervisors, District 3","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":42549,"candidates":[{"candidateName":"Otto Lee","candidateIncumbent":true,"candidateParty":"","voteCount":42549}]},"SCD5":{"id":"SCD5","type":"localRace","location":"Santa Clara","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/santaclara/supervisor-5th-district","raceType":"top2","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":88712,"candidates":[{"candidateName":"Margaret Abe-Koga","candidateIncumbent":false,"candidateParty":"","voteCount":37172},{"candidateName":"Sally J. Lieber","candidateIncumbent":false,"candidateParty":"","voteCount":21962},{"candidateName":"Barry Chang","candidateIncumbent":false,"candidateParty":"","voteCount":6164},{"candidateName":"Peter C. Fung","candidateIncumbent":false,"candidateParty":"","voteCount":17892},{"candidateName":"Sandy Sans","candidateIncumbent":false,"candidateParty":"","voteCount":5522}]},"SCSJMayor":{"id":"SCSJMayor","type":"localRace","location":"Santa Clara","raceName":"San José Mayor","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":167064,"candidates":[{"candidateName":"Matt Mahan","candidateIncumbent":true,"candidateParty":"","voteCount":144701},{"candidateName":"Tyrone Wade","candidateIncumbent":false,"candidateParty":"","voteCount":22363}]},"SCSJD2":{"id":"SCSJD2","type":"localRace","location":"Santa Clara","raceName":"San José City Council, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top2","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":14131,"candidates":[{"candidateName":"Joe Lopez","candidateIncumbent":false,"candidateParty":"","voteCount":4950},{"candidateName":"Pamela Campos","candidateIncumbent":false,"candidateParty":"","voteCount":3436},{"candidateName":"Vanessa Sandoval","candidateIncumbent":false,"candidateParty":"","voteCount":2719},{"candidateName":"Babu Prasad","candidateIncumbent":false,"candidateParty":"","voteCount":3026}]},"SCSJD4":{"id":"SCSJD4","type":"localRace","location":"Santa Clara","raceName":"San José City Council, District 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":14322,"candidates":[{"candidateName":"Kansen Chu","candidateIncumbent":false,"candidateParty":"","voteCount":5931},{"candidateName":"David Cohen","candidateIncumbent":true,"candidateParty":"","voteCount":8391}]},"SCSJD6":{"id":"SCSJD6","type":"localRace","location":"Santa Clara","raceName":"San José City Council, District 6","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top2","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":25108,"candidates":[{"candidateName":"David Cohen","candidateIncumbent":false,"candidateParty":"","voteCount":9875},{"candidateName":"Alex Shoor","candidateIncumbent":false,"candidateParty":"","voteCount":3850},{"candidateName":"Angelo \"A.J.\" Pasciuti","candidateIncumbent":false,"candidateParty":"","voteCount":2688},{"candidateName":"Michael Mulcahy","candidateIncumbent":false,"candidateParty":"","voteCount":8695}]},"SCSJD8":{"id":"SCSJD8","type":"localRace","location":"Santa Clara","raceName":"San José City Council, District 8","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top2","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":21462,"candidates":[{"candidateName":"Tam Truong","candidateIncumbent":false,"candidateParty":"","voteCount":6982},{"candidateName":"Domingo Candelas","candidateIncumbent":true,"candidateParty":"","voteCount":8466},{"candidateName":"Sukhdev Singh Bainiwal","candidateIncumbent":false,"candidateParty":"","voteCount":5513},{"candidateName":"Surinder Kaur Dhaliwal","candidateIncumbent":false,"candidateParty":"","voteCount":501}]},"SCSJD10":{"id":"SCSJD10","type":"localRace","location":"Santa Clara","raceName":"San José City Council, District 10","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top2","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":22799,"candidates":[{"candidateName":"George Casey","candidateIncumbent":false,"candidateParty":"","voteCount":8805},{"candidateName":"Arjun Batra","candidateIncumbent":true,"candidateParty":"","voteCount":8354},{"candidateName":"Lenka Wright","candidateIncumbent":false,"candidateParty":"","voteCount":5640}]},"SCMeasureA":{"id":"SCMeasureA","type":"localRace","location":"Santa Clara","raceName":"Measure A","raceDescription":"Santa Clara. Appointed city clerk. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":20315,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":6580},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":13735}]},"SCMeasureB":{"id":"SCMeasureB","type":"localRace","location":"Santa Clara","raceName":"Measure B","raceDescription":"Santa Clara. Appointed police chief. Passes with majority vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":20567,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":5680},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":14887}]},"SCMeasureC":{"id":"SCMeasureC","type":"localRace","location":"Santa Clara","raceName":"Measure C","raceDescription":"Sunnyvale School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:05 PM","dateUpdated":"April 4, 2024","totalVotes":14656,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":10261},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":4395}]},"SolanoD15":{"id":"SolanoD15","type":"localRace","location":"Solano","raceName":"Superior Court Judge, Department 15","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":81709,"candidates":[{"candidateName":"Mike Thompson","candidateIncumbent":false,"candidateParty":"","voteCount":36844},{"candidateName":"Bryan J. Kim","candidateIncumbent":false,"candidateParty":"","voteCount":44865}]},"SolanoD1":{"id":"SolanoD1","type":"localRace","location":"Solano","raceName":"Board of Supervisors, District 1","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/solano/supervisor-1st-district","raceType":"","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":13786,"candidates":[{"candidateName":"Michael Wilson","candidateIncumbent":false,"candidateParty":"","voteCount":6401},{"candidateName":"Cassandra James","candidateIncumbent":false,"candidateParty":"","voteCount":7385}]},"SolanoD2":{"id":"SolanoD2","type":"localRace","location":"Solano","raceName":"Board of Supervisors, District 2","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":19903,"candidates":[{"candidateName":"Monica Brown","candidateIncumbent":true,"candidateParty":"","voteCount":10951},{"candidateName":"Nora Dizon","candidateIncumbent":false,"candidateParty":"","voteCount":3135},{"candidateName":"Rochelle Sherlock","candidateIncumbent":false,"candidateParty":"","voteCount":5817}]},"SolanoD5":{"id":"SolanoD5","type":"localRace","location":"Solano","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":17888,"candidates":[{"candidateName":"Mitch Mashburn","candidateIncumbent":true,"candidateParty":"","voteCount":11210},{"candidateName":"Chadwick J. Ledoux","candidateIncumbent":false,"candidateParty":"","voteCount":6678}]},"SolanoEducation":{"id":"SolanoEducation","type":"localRace","location":"Solano","raceName":"Sacramento County Board of Education","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":3650,"candidates":[{"candidateName":"Heather Davis","candidateIncumbent":true,"candidateParty":"","voteCount":2960},{"candidateName":"Shazleen Khan","candidateIncumbent":false,"candidateParty":"","voteCount":690}]},"SolanoMeasureA":{"id":"SolanoMeasureA","type":"localRace","location":"Solano","raceName":"Measure A","raceDescription":"Benicia. Hotel tax. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/solano/measure-a","raceType":"yesNo","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":10136,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":7869},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":2267}]},"SolanoMeasureB":{"id":"SolanoMeasureB","type":"localRace","location":"Solano","raceName":"Measure B","raceDescription":"Benicia. Sales tax. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/solano/measure-b","raceType":"yesNo","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":10164,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":7335},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":2829}]},"SolanoMeasureC":{"id":"SolanoMeasureC","type":"localRace","location":"Solano","raceName":"Measure C","raceDescription":"Benicia Unified School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":10112,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":6316},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3796}]},"SolanoMeasureN":{"id":"SolanoMeasureN","type":"localRace","location":"Solano","raceName":"Measure N","raceDescription":"Davis Joint Unified School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"7:08 PM","dateUpdated":"March 28, 2024","totalVotes":15,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":5},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":10}]},"SonomaJudge3":{"id":"SonomaJudge3","type":"localRace","location":"Sonoma","raceName":"Superior Court Judge, Office 3","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":115405,"candidates":[{"candidateName":"Kristine M. Burk","candidateIncumbent":false,"candidateParty":"","voteCount":79498},{"candidateName":"Beki Berrey","candidateIncumbent":false,"candidateParty":"","voteCount":35907}]},"SonomaJudge4":{"id":"SonomaJudge4","type":"localRace","location":"Sonoma","raceName":"Superior Court Judge, Office 4","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":86789,"candidates":[{"candidateName":"Paul J. Lozada","candidateIncumbent":false,"candidateParty":"","voteCount":86789}]},"SonomaJudge6":{"id":"SonomaJudge6","type":"localRace","location":"Sonoma","raceName":"Superior Court Judge, Office 6","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":117990,"candidates":[{"candidateName":"Omar Figueroa","candidateIncumbent":false,"candidateParty":"","voteCount":42236},{"candidateName":"Kenneth English","candidateIncumbent":false,"candidateParty":"","voteCount":75754}]},"SonomaD1":{"id":"SonomaD1","type":"localRace","location":"Sonoma","raceName":"Board of Supervisors, District 1","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":30348,"candidates":[{"candidateName":"Rebecca Hermosillo","candidateIncumbent":false,"candidateParty":"","voteCount":23958},{"candidateName":"Jonathan Mathieu","candidateIncumbent":false,"candidateParty":"","voteCount":6390}]},"SonomaD3":{"id":"SonomaD3","type":"localRace","location":"Sonoma","raceName":"Board of Supervisors, District 3","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"https://www.kqed.org/elections/results/sonoma/supervisor-3rd-district","raceType":"top1","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":16312,"candidates":[{"candidateName":"Chris Coursey","candidateIncumbent":true,"candidateParty":"","voteCount":11346},{"candidateName":"Omar Medina","candidateIncumbent":false,"candidateParty":"","voteCount":4966}]},"SonomaD5":{"id":"SonomaD5","type":"localRace","location":"Sonoma","raceName":"Board of Supervisors, District 5","raceDescription":"Candidate with majority vote wins seat. If no candidate reaches majority, top two candidates advance to runoff in general election.","raceReadTheStory":"","raceType":"top1","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":23356,"candidates":[{"candidateName":"Lynda Hopkins","candidateIncumbent":true,"candidateParty":"","voteCount":23356}]},"SonomaMeasureA":{"id":"SonomaMeasureA","type":"localRace","location":"Sonoma","raceName":"Measure A","raceDescription":"Cotati-Rohnert Park Unified School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":13756,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":10320},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3436}]},"SonomaMeasureB":{"id":"SonomaMeasureB","type":"localRace","location":"Sonoma","raceName":"Measure B","raceDescription":"Petaluma Joint Union High School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":24877,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":15795},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":9082}]},"SonomaMeasureC":{"id":"SonomaMeasureC","type":"localRace","location":"Sonoma","raceName":"Measure C","raceDescription":"Fort Ross School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":286,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":159},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":127}]},"SonomaMeasureD":{"id":"SonomaMeasureD","type":"localRace","location":"Sonoma","raceName":"Measure D","raceDescription":"Harmony Union School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":1925,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":1089},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":836}]},"SonomaMeasureE":{"id":"SonomaMeasureE","type":"localRace","location":"Sonoma","raceName":"Measure E","raceDescription":"Petaluma City (Elementary) School District. Parcel tax. Passes with 2/3 vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":11133,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":7622},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":3511}]},"SonomaMeasureG":{"id":"SonomaMeasureG","type":"localRace","location":"Sonoma","raceName":"Measure G","raceDescription":"Rincon Valley Union School District. School bond. Passes with 55% vote.","raceReadTheStory":"","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":14577,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":8668},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":5909}]},"SonomaMeasureH":{"id":"SonomaMeasureH","type":"localRace","location":"Sonoma","raceName":"Measure H","raceDescription":"Sonoma County. Sales tax. Passes with majority vote.","raceReadTheStory":"https://www.kqed.org/elections/results/sonoma/measure-h","raceType":"yesNo","timeUpdated":"6:51 PM","dateUpdated":"March 29, 2024","totalVotes":145261,"candidates":[{"candidateName":"Yes","candidateIncumbent":false,"candidateParty":"","voteCount":89646},{"candidateName":"No","candidateIncumbent":false,"candidateParty":"","voteCount":55615}]}},"radioSchedulesReducer":{},"listsReducer":{"trending/news,forum?daysPublished=2":{"isFetching":false,"latestQuery":{"from":0,"postsToRender":10},"tag":null,"vitalsOnly":true,"totalRequested":10,"isLoading":false,"isLoadingMore":false,"total":10,"items":["news_11983016","news_11983146","news_11983120","news_11983217","forum_2010101905416","news_11983180","news_11983000","forum_2010101905411","news_11983211","news_11983285"]}},"recallGuideReducer":{"intros":{},"policy":{},"candidates":{}},"savedPostsReducer":{},"pfsSessionReducer":{},"siteSettingsReducer":{},"subscriptionsReducer":{},"termsReducer":{"about":{"name":"About","type":"terms","id":"about","slug":"about","link":"/about","taxonomy":"site"},"arts":{"name":"Arts & Culture","grouping":["arts","pop","trulyca"],"description":"KQED Arts provides daily in-depth coverage of the Bay Area's music, art, film, performing arts, literature and arts news, as well as cultural commentary and criticism.","type":"terms","id":"arts","slug":"arts","link":"/arts","taxonomy":"site"},"artschool":{"name":"Art School","parent":"arts","type":"terms","id":"artschool","slug":"artschool","link":"/artschool","taxonomy":"site"},"bayareabites":{"name":"KQED food","grouping":["food","bayareabites","checkplease"],"parent":"food","type":"terms","id":"bayareabites","slug":"bayareabites","link":"/food","taxonomy":"site"},"bayareahiphop":{"name":"Bay Area Hiphop","type":"terms","id":"bayareahiphop","slug":"bayareahiphop","link":"/bayareahiphop","taxonomy":"site"},"campaign21":{"name":"Campaign 21","type":"terms","id":"campaign21","slug":"campaign21","link":"/campaign21","taxonomy":"site"},"checkplease":{"name":"KQED food","grouping":["food","bayareabites","checkplease"],"parent":"food","type":"terms","id":"checkplease","slug":"checkplease","link":"/food","taxonomy":"site"},"education":{"name":"Education","grouping":["education"],"type":"terms","id":"education","slug":"education","link":"/education","taxonomy":"site"},"elections":{"name":"Elections","type":"terms","id":"elections","slug":"elections","link":"/elections","taxonomy":"site"},"events":{"name":"Events","type":"terms","id":"events","slug":"events","link":"/events","taxonomy":"site"},"event":{"name":"Event","alias":"events","type":"terms","id":"event","slug":"event","link":"/event","taxonomy":"site"},"filmschoolshorts":{"name":"Film School Shorts","type":"terms","id":"filmschoolshorts","slug":"filmschoolshorts","link":"/filmschoolshorts","taxonomy":"site"},"food":{"name":"KQED food","grouping":["food","bayareabites","checkplease"],"type":"terms","id":"food","slug":"food","link":"/food","taxonomy":"site"},"forum":{"name":"Forum","relatedContentQuery":"posts/forum?","parent":"news","type":"terms","id":"forum","slug":"forum","link":"/forum","taxonomy":"site"},"futureofyou":{"name":"Future of You","grouping":["science","futureofyou"],"parent":"science","type":"terms","id":"futureofyou","slug":"futureofyou","link":"/futureofyou","taxonomy":"site"},"jpepinheart":{"name":"KQED food","relatedContentQuery":"trending/food,bayareabites,checkplease","parent":"food","type":"terms","id":"jpepinheart","slug":"jpepinheart","link":"/food","taxonomy":"site"},"liveblog":{"name":"Live Blog","type":"terms","id":"liveblog","slug":"liveblog","link":"/liveblog","taxonomy":"site"},"livetv":{"name":"Live TV","parent":"tv","type":"terms","id":"livetv","slug":"livetv","link":"/livetv","taxonomy":"site"},"lowdown":{"name":"The Lowdown","relatedContentQuery":"posts/lowdown?","parent":"news","type":"terms","id":"lowdown","slug":"lowdown","link":"/lowdown","taxonomy":"site"},"mindshift":{"name":"Mindshift","parent":"news","description":"MindShift explores the future of education by highlighting the innovative – and sometimes counterintuitive – ways educators and parents are helping all children succeed.","type":"terms","id":"mindshift","slug":"mindshift","link":"/mindshift","taxonomy":"site"},"news":{"name":"News","grouping":["news","forum"],"type":"terms","id":"news","slug":"news","link":"/news","taxonomy":"site"},"perspectives":{"name":"Perspectives","parent":"radio","type":"terms","id":"perspectives","slug":"perspectives","link":"/perspectives","taxonomy":"site"},"podcasts":{"name":"Podcasts","type":"terms","id":"podcasts","slug":"podcasts","link":"/podcasts","taxonomy":"site"},"pop":{"name":"Pop","parent":"arts","type":"terms","id":"pop","slug":"pop","link":"/pop","taxonomy":"site"},"pressroom":{"name":"Pressroom","type":"terms","id":"pressroom","slug":"pressroom","link":"/pressroom","taxonomy":"site"},"quest":{"name":"Quest","parent":"science","type":"terms","id":"quest","slug":"quest","link":"/quest","taxonomy":"site"},"radio":{"name":"Radio","grouping":["forum","perspectives"],"description":"Listen to KQED Public Radio – home of Forum and The California Report – on 88.5 FM in San Francisco, 89.3 FM in Sacramento, 88.3 FM in Santa Rosa and 88.1 FM in Martinez.","type":"terms","id":"radio","slug":"radio","link":"/radio","taxonomy":"site"},"root":{"name":"KQED","image":"https://ww2.kqed.org/app/uploads/2020/02/KQED-OG-Image@1x.png","imageWidth":1200,"imageHeight":630,"headData":{"title":"KQED | News, Radio, Podcasts, TV | Public Media for Northern California","description":"KQED provides public radio, television, and independent reporting on issues that matter to the Bay Area. We’re the NPR and PBS member station for Northern California."},"type":"terms","id":"root","slug":"root","link":"/root","taxonomy":"site"},"science":{"name":"Science","grouping":["science","futureofyou"],"description":"KQED Science brings you award-winning science and environment coverage from the Bay Area and beyond.","type":"terms","id":"science","slug":"science","link":"/science","taxonomy":"site"},"stateofhealth":{"name":"State of Health","parent":"science","type":"terms","id":"stateofhealth","slug":"stateofhealth","link":"/stateofhealth","taxonomy":"site"},"support":{"name":"Support","type":"terms","id":"support","slug":"support","link":"/support","taxonomy":"site"},"thedolist":{"name":"The Do List","parent":"arts","type":"terms","id":"thedolist","slug":"thedolist","link":"/thedolist","taxonomy":"site"},"trulyca":{"name":"Truly CA","grouping":["arts","pop","trulyca"],"parent":"arts","type":"terms","id":"trulyca","slug":"trulyca","link":"/trulyca","taxonomy":"site"},"tv":{"name":"TV","type":"terms","id":"tv","slug":"tv","link":"/tv","taxonomy":"site"},"voterguide":{"name":"Voter Guide","parent":"elections","alias":"elections","type":"terms","id":"voterguide","slug":"voterguide","link":"/voterguide","taxonomy":"site"},"source_news_11983211":{"type":"terms","id":"source_news_11983211","meta":{"override":true},"name":"Morning Report","link":"https://www.kqed.org/news/tag/tcrarchive/","isLoading":false},"news_72":{"type":"terms","id":"news_72","meta":{"index":"terms_1591234321","site":"news","id":"72","found":true},"relationships":{},"included":{},"name":"The California Report","slug":"the-california-report","taxonomy":"program","description":null,"featImg":"https://ww2.kqed.org/app/uploads/sites/10/2014/10/TCR-2-Logo-Web-Banners-03.png","headData":{"title":"The California Report Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":6969,"isLoading":false,"link":"/news/program/the-california-report"},"news_8":{"type":"terms","id":"news_8","meta":{"index":"terms_1591234321","site":"news","id":"8","found":true},"relationships":{},"included":{},"name":"News","slug":"news","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"News Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":8,"isLoading":false,"link":"/news/category/news"},"news_22570":{"type":"terms","id":"news_22570","meta":{"index":"terms_1591234321","site":"news","id":"22570","found":true},"relationships":{},"included":{},"name":"early childhood education","slug":"early-childhood-education","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"early childhood education Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":22587,"isLoading":false,"link":"/news/tag/early-childhood-education"},"news_32102":{"type":"terms","id":"news_32102","meta":{"index":"terms_1591234321","site":"news","id":"32102","found":true},"relationships":{},"included":{},"name":"early childhood education and care","slug":"early-childhood-education-and-care","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"early childhood education and care Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":32119,"isLoading":false,"link":"/news/tag/early-childhood-education-and-care"},"news_20013":{"type":"terms","id":"news_20013","meta":{"index":"terms_1591234321","site":"news","id":"20013","found":true},"relationships":{},"included":{},"name":"education","slug":"education","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"education Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":20030,"isLoading":false,"link":"/news/tag/education"},"news_27626":{"type":"terms","id":"news_27626","meta":{"index":"terms_1591234321","site":"news","id":"27626","found":true},"relationships":{},"included":{},"name":"featured-news","slug":"featured-news","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"featured-news Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":27643,"isLoading":false,"link":"/news/tag/featured-news"},"news_17763":{"type":"terms","id":"news_17763","meta":{"index":"terms_1591234321","site":"news","id":"17763","found":true},"relationships":{},"included":{},"name":"preschool","slug":"preschool","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"preschool Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":17797,"isLoading":false,"link":"/news/tag/preschool"},"news_33746":{"type":"terms","id":"news_33746","meta":{"index":"terms_1591234321","site":"news","id":"33746","found":true},"relationships":{},"included":{},"name":"Education","slug":"education","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"Education Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33763,"isLoading":false,"link":"/news/interest/education"},"news_33733":{"type":"terms","id":"news_33733","meta":{"index":"terms_1591234321","site":"news","id":"33733","found":true},"relationships":{},"included":{},"name":"News","slug":"news","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"News Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33750,"isLoading":false,"link":"/news/interest/news"},"news_25314":{"type":"terms","id":"news_25314","meta":{"index":"terms_1591234321","site":"news","id":"25314","found":true},"relationships":{},"included":{},"name":"overnight RV parking","slug":"overnight-rv-parking","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"overnight RV parking Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":25331,"isLoading":false,"link":"/news/tag/overnight-rv-parking"},"news_24635":{"type":"terms","id":"news_24635","meta":{"index":"terms_1591234321","site":"news","id":"24635","found":true},"relationships":{},"included":{},"name":"RVs","slug":"rvs","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"RVs Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":24652,"isLoading":false,"link":"/news/tag/rvs"},"news_31793":{"type":"terms","id":"news_31793","meta":{"index":"terms_1591234321","site":"news","id":"31793","found":true},"relationships":{},"included":{},"name":"unhoused residents","slug":"unhoused-residents","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"unhoused residents Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":31810,"isLoading":false,"link":"/news/tag/unhoused-residents"},"news_10":{"type":"terms","id":"news_10","meta":{"index":"terms_1591234321","site":"news","id":"10","found":true},"relationships":{},"included":{},"name":"Sports","slug":"sports","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"Sports Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":10,"isLoading":false,"link":"/news/category/sports"},"news_32793":{"type":"terms","id":"news_32793","meta":{"index":"terms_1591234321","site":"news","id":"32793","found":true},"relationships":{},"included":{},"name":"Bay Area soccer","slug":"bay-area-soccer","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"Bay Area soccer Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":32810,"isLoading":false,"link":"/news/tag/bay-area-soccer"},"news_18":{"type":"terms","id":"news_18","meta":{"index":"terms_1591234321","site":"news","id":"18","found":true},"relationships":{},"included":{},"name":"Oakland","slug":"oakland","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"Oakland Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":86,"isLoading":false,"link":"/news/tag/oakland"},"news_38":{"type":"terms","id":"news_38","meta":{"index":"terms_1591234321","site":"news","id":"38","found":true},"relationships":{},"included":{},"name":"San Francisco","slug":"san-francisco","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"San Francisco Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":58,"isLoading":false,"link":"/news/tag/san-francisco"},"news_111":{"type":"terms","id":"news_111","meta":{"index":"terms_1591234321","site":"news","id":"111","found":true},"relationships":{},"included":{},"name":"sports","slug":"sports-2","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"sports Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":115,"isLoading":false,"link":"/news/tag/sports-2"},"news_26124":{"type":"terms","id":"news_26124","meta":{"index":"terms_1591234321","site":"news","id":"26124","found":true},"relationships":{},"included":{},"name":"U.S. Soccer","slug":"u-s-soccer","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"U.S. Soccer Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":26141,"isLoading":false,"link":"/news/tag/u-s-soccer"},"news_28623":{"type":"terms","id":"news_28623","meta":{"index":"terms_1591234321","site":"news","id":"28623","found":true},"relationships":{},"included":{},"name":"women's soccer","slug":"womens-soccer","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"women's soccer Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":28640,"isLoading":false,"link":"/news/tag/womens-soccer"},"news_33741":{"type":"terms","id":"news_33741","meta":{"index":"terms_1591234321","site":"news","id":"33741","found":true},"relationships":{},"included":{},"name":"East Bay","slug":"east-bay","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"East Bay Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33758,"isLoading":false,"link":"/news/interest/east-bay"},"news_33749":{"type":"terms","id":"news_33749","meta":{"index":"terms_1591234321","site":"news","id":"33749","found":true},"relationships":{},"included":{},"name":"Entertainment","slug":"entertainment","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"Entertainment Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33766,"isLoading":false,"link":"/news/interest/entertainment"},"news_33740":{"type":"terms","id":"news_33740","meta":{"index":"terms_1591234321","site":"news","id":"33740","found":true},"relationships":{},"included":{},"name":"Events","slug":"events","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"Events Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33757,"isLoading":false,"link":"/news/interest/events"},"news_33729":{"type":"terms","id":"news_33729","meta":{"index":"terms_1591234321","site":"news","id":"33729","found":true},"relationships":{},"included":{},"name":"San Francisco","slug":"san-francisco","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"San Francisco Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33746,"isLoading":false,"link":"/news/interest/san-francisco"},"news_457":{"type":"terms","id":"news_457","meta":{"index":"terms_1591234321","site":"news","id":"457","found":true},"relationships":{},"included":{},"name":"Health","slug":"health","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"Health Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":16998,"isLoading":false,"link":"/news/category/health"},"news_18538":{"type":"terms","id":"news_18538","meta":{"index":"terms_1591234321","site":"news","id":"18538","found":true},"relationships":{},"included":{},"name":"California","slug":"california","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"California Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":31,"isLoading":false,"link":"/news/tag/california"},"news_18543":{"type":"terms","id":"news_18543","meta":{"index":"terms_1591234321","site":"news","id":"18543","found":true},"relationships":{},"included":{},"name":"Health","slug":"health","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"Health Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":466,"isLoading":false,"link":"/news/tag/health"},"news_18659":{"type":"terms","id":"news_18659","meta":{"index":"terms_1591234321","site":"news","id":"18659","found":true},"relationships":{},"included":{},"name":"hospitals","slug":"hospitals","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"hospitals Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":18676,"isLoading":false,"link":"/news/tag/hospitals"},"news_33578":{"type":"terms","id":"news_33578","meta":{"index":"terms_1591234321","site":"news","id":"33578","found":true},"relationships":{},"included":{},"name":"maternity care","slug":"maternity-care","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"maternity care Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33595,"isLoading":false,"link":"/news/tag/maternity-care"},"news_21771":{"type":"terms","id":"news_21771","meta":{"index":"terms_1591234321","site":"news","id":"21771","found":true},"relationships":{},"included":{},"name":"pregnancy","slug":"pregnancy","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"pregnancy Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":21788,"isLoading":false,"link":"/news/tag/pregnancy"},"news_33583":{"type":"terms","id":"news_33583","meta":{"index":"terms_1591234321","site":"news","id":"33583","found":true},"relationships":{},"included":{},"name":"pregnancy-related deaths","slug":"pregnancy-related-deaths","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"pregnancy-related deaths Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33600,"isLoading":false,"link":"/news/tag/pregnancy-related-deaths"},"news_18481":{"type":"terms","id":"news_18481","meta":{"index":"terms_1591234321","site":"news","id":"18481","found":true},"relationships":{},"included":{},"name":"CALmatters","slug":"calmatters","taxonomy":"affiliate","description":null,"featImg":null,"headData":{"title":"CALmatters Archives | KQED Arts","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":18515,"isLoading":false,"link":"/news/affiliate/calmatters"},"news_33747":{"type":"terms","id":"news_33747","meta":{"index":"terms_1591234321","site":"news","id":"33747","found":true},"relationships":{},"included":{},"name":"Health","slug":"health","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"Health Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33764,"isLoading":false,"link":"/news/interest/health"},"forum_165":{"type":"terms","id":"forum_165","meta":{"index":"terms_1591234321","site":"forum","id":"165","found":true},"relationships":{},"included":{},"name":"Default","slug":"default","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"Default Archives | KQED Forum","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":165,"isLoading":false,"link":"/forum/category/default"},"news_6266":{"type":"terms","id":"news_6266","meta":{"index":"terms_1591234321","site":"news","id":"6266","found":true},"relationships":{},"included":{},"name":"Housing","slug":"housing","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"Housing Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":6290,"isLoading":false,"link":"/news/category/housing"},"news_22307":{"type":"terms","id":"news_22307","meta":{"index":"terms_1591234321","site":"news","id":"22307","found":true},"relationships":{},"included":{},"name":"california laws","slug":"california-laws","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"california laws Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":22324,"isLoading":false,"link":"/news/tag/california-laws"},"news_33966":{"type":"terms","id":"news_33966","meta":{"index":"terms_1591234321","site":"news","id":"33966","found":true},"relationships":{},"included":{},"name":"encampment ban","slug":"encampment-ban","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"encampment ban Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33983,"isLoading":false,"link":"/news/tag/encampment-ban"},"news_21214":{"type":"terms","id":"news_21214","meta":{"index":"terms_1591234321","site":"news","id":"21214","found":true},"relationships":{},"included":{},"name":"homeless encampments","slug":"homeless-encampments","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"homeless encampments Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":21231,"isLoading":false,"link":"/news/tag/homeless-encampments"},"news_4020":{"type":"terms","id":"news_4020","meta":{"index":"terms_1591234321","site":"news","id":"4020","found":true},"relationships":{},"included":{},"name":"homelessness","slug":"homelessness","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"homelessness Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":4039,"isLoading":false,"link":"/news/tag/homelessness"},"news_1775":{"type":"terms","id":"news_1775","meta":{"index":"terms_1591234321","site":"news","id":"1775","found":true},"relationships":{},"included":{},"name":"housing","slug":"housing","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"housing Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":1790,"isLoading":false,"link":"/news/tag/housing"},"news_33739":{"type":"terms","id":"news_33739","meta":{"index":"terms_1591234321","site":"news","id":"33739","found":true},"relationships":{},"included":{},"name":"Housing","slug":"housing","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"Housing Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33756,"isLoading":false,"link":"/news/interest/housing"},"news_32695":{"type":"terms","id":"news_32695","meta":{"index":"terms_1591234321","site":"news","id":"32695","found":true},"relationships":{},"included":{},"name":"construction","slug":"construction","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"construction Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":32712,"isLoading":false,"link":"/news/tag/construction"},"news_17620":{"type":"terms","id":"news_17620","meta":{"index":"terms_1591234321","site":"news","id":"17620","found":true},"relationships":{},"included":{},"name":"developers","slug":"developers","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"developers Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":17654,"isLoading":false,"link":"/news/tag/developers"},"news_423":{"type":"terms","id":"news_423","meta":{"index":"terms_1591234321","site":"news","id":"423","found":true},"relationships":{},"included":{},"name":"taxes","slug":"taxes","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"taxes Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":432,"isLoading":false,"link":"/news/tag/taxes"},"news_21291":{"type":"terms","id":"news_21291","meta":{"index":"terms_1591234321","site":"news","id":"21291","found":true},"relationships":{},"included":{},"name":"Uncategorized","slug":"uncategorized","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"Uncategorized Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":21308,"isLoading":false,"link":"/news/category/uncategorized"},"news_21998":{"type":"terms","id":"news_21998","meta":{"index":"terms_1591234321","site":"news","id":"21998","found":true},"relationships":{},"included":{},"name":"TCRAM","slug":"tcram","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"TCRAM Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":22015,"isLoading":false,"link":"/news/tag/tcram"},"news_21268":{"type":"terms","id":"news_21268","meta":{"index":"terms_1591234321","site":"news","id":"21268","found":true},"relationships":{},"included":{},"name":"tcrarchive","slug":"tcrarchive","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"tcrarchive Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":21285,"isLoading":false,"link":"/news/tag/tcrarchive"},"news_32222":{"type":"terms","id":"news_32222","meta":{"index":"terms_1591234321","site":"news","id":"32222","found":true},"relationships":{},"included":{},"name":"California prison","slug":"california-prison","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"California prison Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":32239,"isLoading":false,"link":"/news/tag/california-prison"},"news_33888":{"type":"terms","id":"news_33888","meta":{"index":"terms_1591234321","site":"news","id":"33888","found":true},"relationships":{},"included":{},"name":"Federal Correctional Institution in Dublin","slug":"federal-correctional-institution-in-dublin","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"Federal Correctional Institution in Dublin Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33905,"isLoading":false,"link":"/news/tag/federal-correctional-institution-in-dublin"},"news_33745":{"type":"terms","id":"news_33745","meta":{"index":"terms_1591234321","site":"news","id":"33745","found":true},"relationships":{},"included":{},"name":"Criminal Justice","slug":"criminal-justice","taxonomy":"interest","description":null,"featImg":null,"headData":{"title":"Criminal Justice Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":33762,"isLoading":false,"link":"/news/interest/criminal-justice"},"news_356":{"type":"terms","id":"news_356","meta":{"index":"terms_1591234321","site":"news","id":"356","found":true},"relationships":{},"included":{},"name":"Science","slug":"science","taxonomy":"category","description":null,"featImg":null,"headData":{"title":"Science Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":364,"isLoading":false,"link":"/news/category/science"},"news_21434":{"type":"terms","id":"news_21434","meta":{"index":"terms_1591234321","site":"news","id":"21434","found":true},"relationships":{},"included":{},"name":"addiction","slug":"addiction","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"addiction Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":21451,"isLoading":false,"link":"/news/tag/addiction"},"news_25076":{"type":"terms","id":"news_25076","meta":{"index":"terms_1591234321","site":"news","id":"25076","found":true},"relationships":{},"included":{},"name":"meth","slug":"meth","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"meth Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":25093,"isLoading":false,"link":"/news/tag/meth"},"news_24982":{"type":"terms","id":"news_24982","meta":{"index":"terms_1591234321","site":"news","id":"24982","found":true},"relationships":{},"included":{},"name":"methamphetamine","slug":"methamphetamine","taxonomy":"tag","description":null,"featImg":null,"headData":{"title":"methamphetamine Archives | KQED News","description":null,"ogTitle":null,"ogDescription":null,"ogImgId":null,"twTitle":null,"twDescription":null,"twImgId":null},"ttid":24999,"isLoading":false,"link":"/news/tag/methamphetamine"}},"userAgentReducer":{"userAgent":"claudebot","isBot":true},"userPermissionsReducer":{"wpLoggedIn":false},"localStorageReducer":{},"browserHistoryReducer":[],"eventsReducer":{},"fssReducer":{},"tvDailyScheduleReducer":{},"tvWeeklyScheduleReducer":{},"tvPrimetimeScheduleReducer":{},"tvMonthlyScheduleReducer":{},"userAccountReducer":{"routeTo":"","showDeleteConfirmModal":false,"user":{"userId":"","isFound":false,"firstName":"","lastName":"","phoneNumber":"","email":"","articles":[]}},"youthMediaReducer":{},"checkPleaseReducer":{"filterData":{},"restaurantData":[]},"reframeReducer":{"attendee":null},"location":{"pathname":"/news/11728856/stanford-researchers-using-mri-scans-to-predict-meth-and-cocaine-relapse?utm_source=March+1%2C+2019+Newsletter&utm_campaign=March+1%2C+2019&utm_medium=email","previousPathname":"/"}}